Strangulated appendiceal intussusception caused by isolated endometriosis
Article information

A 33-year-old female was admitted to our emergency department for right lower quadrant abdominal pain, which was not associated with her menstrual cycle, and nausea, which had persisted for 3 days. She denied any prior history of abdominal pain, dysmenorrhea, menorrhagia, or dyspareunia. The patient had no family history of endometriosis. Abdominal computed tomography revealed appendiceal intussusception (AI) and invagination of the periappendiceal fat into the cecum (Fig. 1). She underwent laparoscopic partial cecectomy with the presumed diagnosis of AI (Fig. 2). The ovaries and fallopian tubes were normal, with no endometrial spot. The inverted appendix was completely necrotic (Fig. 3). Final surgical pathology was positive for gangrenous intussusception of the appendix, with endometrial deposits (Fig. 4).
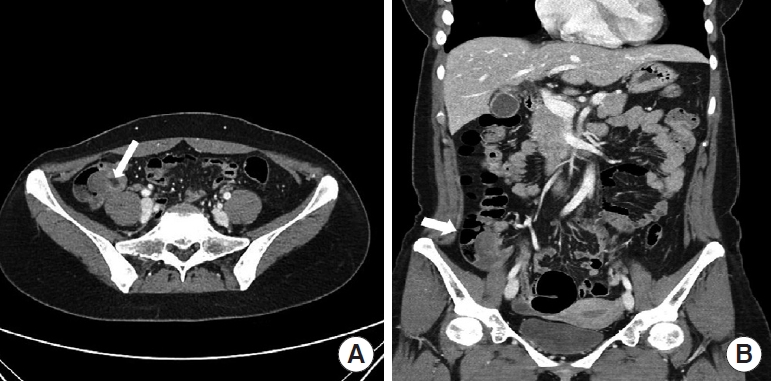
The abdominal computed tomography. (A) Axial view and (B) coronal view. These images show a low-density tubular structure (5×1.6 cm in diameter) in the cecum near the appendiceal orifice, and focal invagination of the peri-appendiceal fat to the cecum (white arrow).

Surgical findings. During laparoscopic exploration, the appendix was not macroscopically visible in the right iliac fossa, but it was located in the cecum (white arrow), which showed no possibility for reduction (black arrow). Terminal ileum denoted by asterisk.

Surgical specimen. Appearance of the specimen resected by laparoscopic partial cecectomy. The inverted appendix (70×15 mm in size) is completely necrotic at the appendiceal orifice (inside the aspect of the cecum denoted by a white arrow).
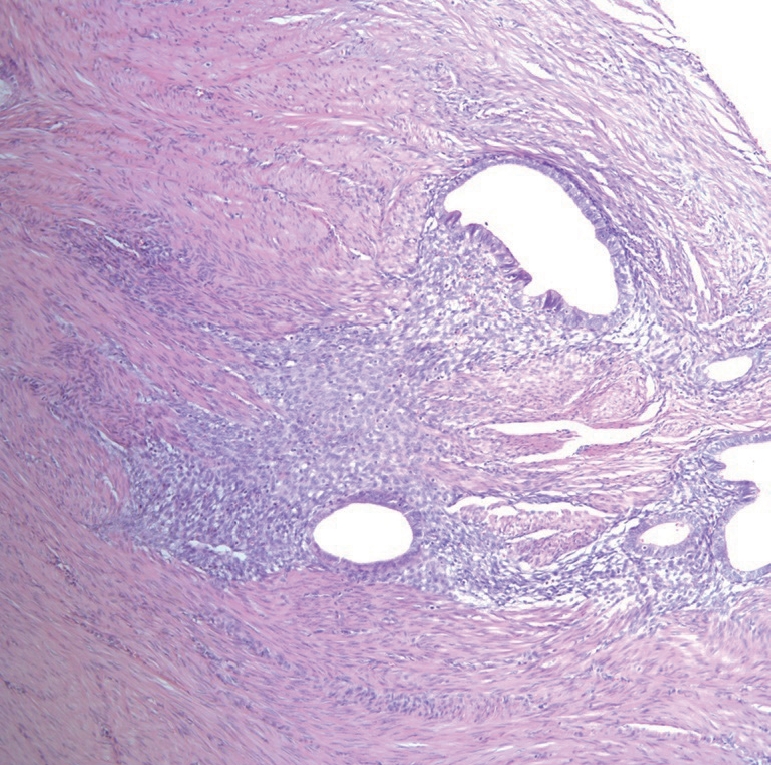
High-power view of endometriosis within the appendix. Endometrial glands and stroma within the muscular layer, around the appendicular mucosa (hematoxylin and eosin, ×200).
Adult colonic intussusception is caused by either malignant tumors (64%–87% cases) or benign tumors (29%–33%). The most common causes are adenocarcinomas and lymphomas among malignant tumors and lipomas, leiomyomas, adenomatous polyps, and endometriosis among benign tumors [1]. AI is extremely rare, with reported rates of 0.01% in patients who undergo appendectomy [2]. AI secondary to endometriosis is also extremely rare, with less than 30 cases reported. However, those cases involved endometriosis on other organs and the appendix. Only three cases involving isolated appendiceal endometriosis are reported in the literatures [3]. Patients with AI can range from being asymptomatic to presenting symptoms mimicking acute appendicitis [4]. Preoperative diagnosis is difficult owing to its rarity. Although endometriosis is reported to be the lead point of AI, there are limited descriptions on imaging findings. Computed tomography findings include an enlarged appendix with an inverted appendiceal tip or a tumor protruding into the cecum [5]. This case highlights that isolated endometriosis without involvement of reproductive organs can present as a strangulated AI. AI secondary to endometriosis should be considered in the differential diagnosis when female patients of childbearing age present with clinical symptoms of acute appendicitis and radiologic findings of intussusception, even before obtaining a pathological result.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This paper was supported by Wonkwang University in 2020.
References
Article information Continued
Notes
Capsule Summary
What is already known
Appendiceal endometriosis can present strangulated intussusception.
What is new in the current study
Appendiceal intussusception secondary to endometriosis should be considered in the differential diagnosis when female patients of reproductive age present with clinical symptoms of acute appendicitis.