INTRODUCTION
The ingestion of esophageal foreign bodies (EFBs) commonly occurs in the pediatric population. Radiography is a reliable diagnostic tool for these cases because commonly ingested foreign bodies, including coins, toys, and bones, are radiopaque. However, in some cases, children ingest organic matter, such as food, which is radiolucent [1]. A rare case of food impaction diagnosed through point-of-care ultrasonography (POCUS) is discussed in the present study.
CASE REPORT
A previously healthy 1-year-old boy suddenly began coughing while eating a dried sweet potato. Because he continued gagging after vomiting a piece of the potato, his mother brought him to our emergency room.
Upon physical examination, the patient was alert with a respiratory rate of 36 breaths per minute and a heart rate of 127 beats per minute. His oxygen saturation was 96% on room air, and his body temperature was 36.5°C. Although respiratory distress was ruled out and his pulmonary examination was normal, he was drooling and gagging.
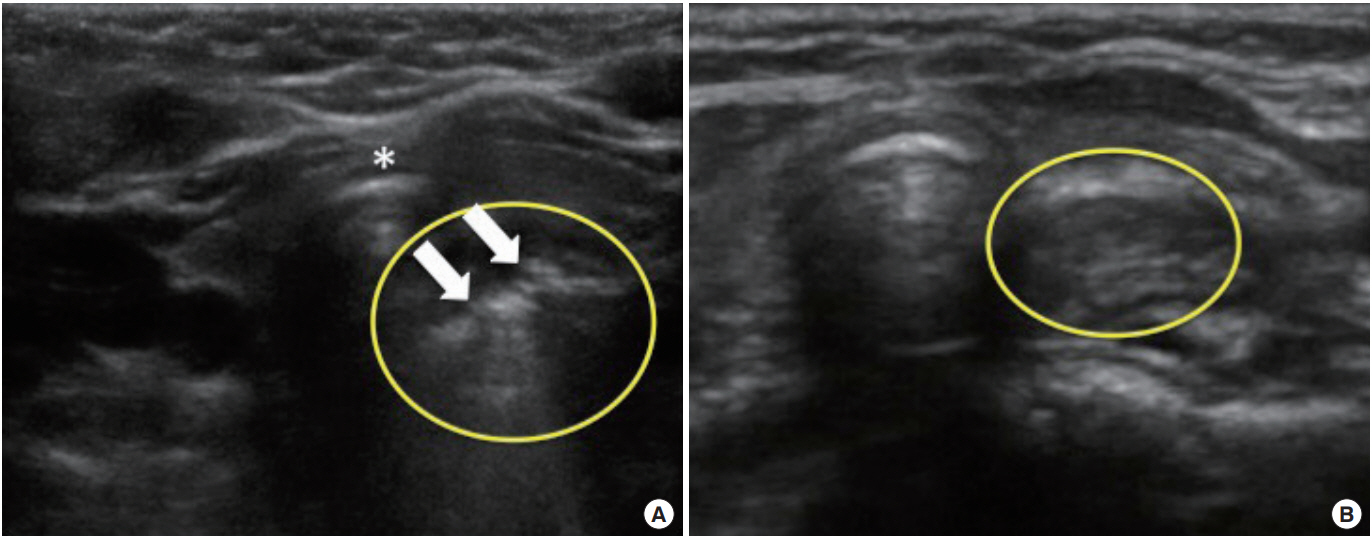
Based on his medical history and physical examination, food impaction at the upper esophagus was suspected. POCUS was performed to detect the ingested foreign body, and it was carried out by placing a linear transducer transversally on the anterior neck and then scanning the thyroid cartilage at the suprasternal notch. Results showed that a linear hyperechoic lesion was obstructing the posterior esophageal wall. The lesion did not move during swallowing (Fig. 1A). Therefore, computed tomography (CT) scanning was considered for a detailed examination of the foreign body prior to emergency removal because plain radiography was not capable of visualizing organic matter. However, the patient vomited the object before CT was performed.
After the object was removed, the patient stopped gagging, and the ultrasonographic findings were normal (Fig. 1B). Thus, the patient was discharged without any complications. Prior to leaving the hospital, his parents were educated on injury prevention.
DISCUSSION
EFBs lodge primarily in any of these three sites, including the esophageal orifice, aortic arch, and lower esophageal sphincter, all of which are characterized by a structural narrowing of the esophageal lumen. However, most foreign bodies obstruct the esophageal orifice [2]. Although coins, batteries, and similar objects are considered as common foreign bodies, the ingestion of other X-ray permeable objects, such as food and plastic items, is also common. CT is a sensitive modality for identifying EFBs. However, this test should be the last resort to avoid radiation exposure, which may enhance the patient’s lifetime risk for malignancies [3]. POCUS is a simple, non-invasive technique that does not use radiation and can detect even permeable objects. Moreover, it is an effective modality for detecting EFBs, particularly radiolucent objects, although the impaction site needs to be considered.
The management of EFBs depends on the location of impaction, object size, its composition, and the patient’s condition [4]. In cases of esophageal food impaction, emergency endoscopic removal of the object is needed if the patient is symptomatic or shows signs of esophageal obstruction, such as drooling [4]. Endoscopic removal is a safe and effective method for treating esophageal food impaction, although the patient’s airway should be secured prior to the procedure [5]. Katsinelos et al. [6] showed that the success rate of endoscopic retrieval in 139 patients with a foreign body obstructed at the upper gastrointestinal tract was 98.6%, and no procedure-related complications were recognized. In the present case, emergency endoscopic removal was indicated due to the patient’s symptoms, which suggested an esophageal obstruction. Fortunately, the patient vomited the foreign body before the procedure. Although a bougie dilator can be used to advance a foreign object into the stomach as an alternative to endoscopic removal, it is not recommended for esophageal food impaction due to the risk of esophageal perforation [4,5].
Reports on the use of POCUS for this purpose are extremely limited. However, Salmon and Doniger [7] successfully used POCUS to detect a foreign body at the first narrowing of the esophagus in a child who was asymptomatic upon hospital arrival. Moreover, Singleton et al. [8] published a case series on the successful detection of food impaction in adults, and Simone et al. [9] reported numerous pediatric cases. Although further studies are needed to fully assess its efficacy, this technique may be effective in diagnosing EFBs, particularly radiopaque objects, while avoiding radiation exposure.