Dear Editor,
The pit viper, which belongs to the Viperidae family, is the most common venomous snake in Northeast Asia [1]. This snakeŌĆÖs venom does not severely affect the human body, and most victims only experience mild to severe local symptoms such as pain, swelling, and necrosis in the bite area [1,2]. Although antivenom therapy is available for fatal snakebite treatment, it offers little to no protection against local effects such as dermonecrosis, myonecrosis, edema, hemorrhage, and inflammation in the bite region [1,2]. Local symptoms can result in serious complications such as compartment syndrome and rhabdomyolysis. Swelling in the bite region is a common and major cause of serious complications for which negative pressure wound therapy has been shown effective [2ŌĆō6]. However, a definitive treatment has yet to be determined.
Vitis vinifera seed extract (VVse) has been studied as an antivenom for snakebites and is useful for neutralization of various venom-induced activities [3ŌĆō6]. It is reportedly effective in the treatment of bites by snakes from the Viperidae family and RussellŌĆÖs and hump-nosed vipers [3ŌĆō6]. The local effects of viper bites can be treated with VVse through neutralization of the venomŌĆÖs edema-inducing and myonecrotic properties. VVse has been reported to abolish hyaluronidase and proteolytic activities, neutralizes hemorrhage, and partially inhibits procoagulant activity attributed to viper venom [3ŌĆō6].
We report two cases of successful treatment of snakebites with VVse. The first patient was treated for ascites that passed through the groin to the abdomen, resulting in increased severe leg swelling following a snakebite. The second patient exhibited hypersensitivity to the antivenom.
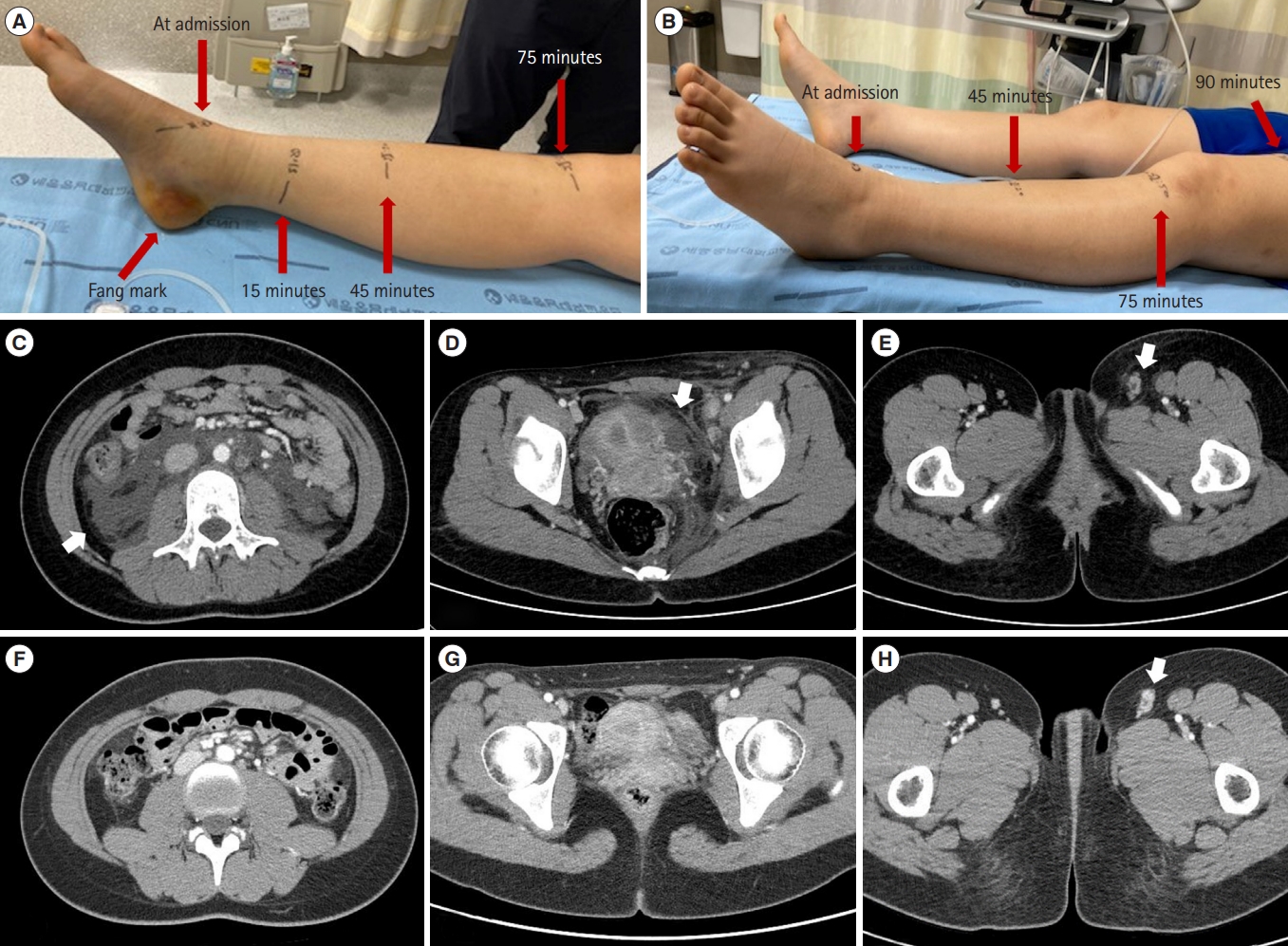
The first case was a 15-year-old female patient with no past medical history admitted for a snakebite on the left heel. She had severe localized pain followed by swelling and bruising of the foot. The patient arrived at the emergency department of a local hospital 10 minutes following the snakebite, with progressive swelling of her left leg and ecchymosis around the fang marks. Kovax freeze-dried Gloydius brevicaudus antivenom 6,000 units (6,000 units/vial, Korea Vaccine) was injected intravenously immediately after arrival at the hospital. A splint was applied for immobilization. The patient reported generalized abdominal pain but no bleeding from the gums, epistaxis, hemoptysis, hematemesis, melena, vaginal bleeding, breathing difficulty, focal neurological deficit, or loss of consciousness. The swelling progressed rapidly to the knee within the 1st hour and proximally to the hip and inguinal area within 2 hours (Fig. 1). The local effect score was 13 (pain, 4; swelling, 4; ecchymosis, 2; time, 3). In addition, the patient developed marked pain in her leg up to her lower abdomen, which progressed to marked generalized abdominal pain one day after admission.
On the second day of admission, abdominopelvic computed tomography (APCT) revealed ascites throughout the abdomen and destructive lymphadenopathy in the femoral and inguinal areas (Fig. 1). The patient was referred to Chungnum National University Sejong Hospital, where laboratory test results revealed no remarkable abnormalities (Table 1). VVse (Entelon, Hanlim Pharm) 300 mg/day (150 mg tablet twice daily) was administered to the patient on the 2nd day following the snakebite. Her symptoms significantly improved on the 4th day, the 2nd day after VVse administration. On the 5th day after the snakebite, the 3rd day after VVse administration, ascites was no longer observed on abdominal ultrasound, and the swelling in the left leg improved, reaching only to the ankle. On the 7th day after the snakebite, the left leg swelling completely resolved, and APCT revealed no definite ascites in the abdomen (Fig. 1). Furthermore, laboratory test results revealed no remarkable changes (Table 1). On the 8th day of the snakebite, the patient was discharged from the hospital. VVse was administered for an additional 6 days after discharge. No specific findings were observed at the outpatient clinic 3 weeks after the snakebite.
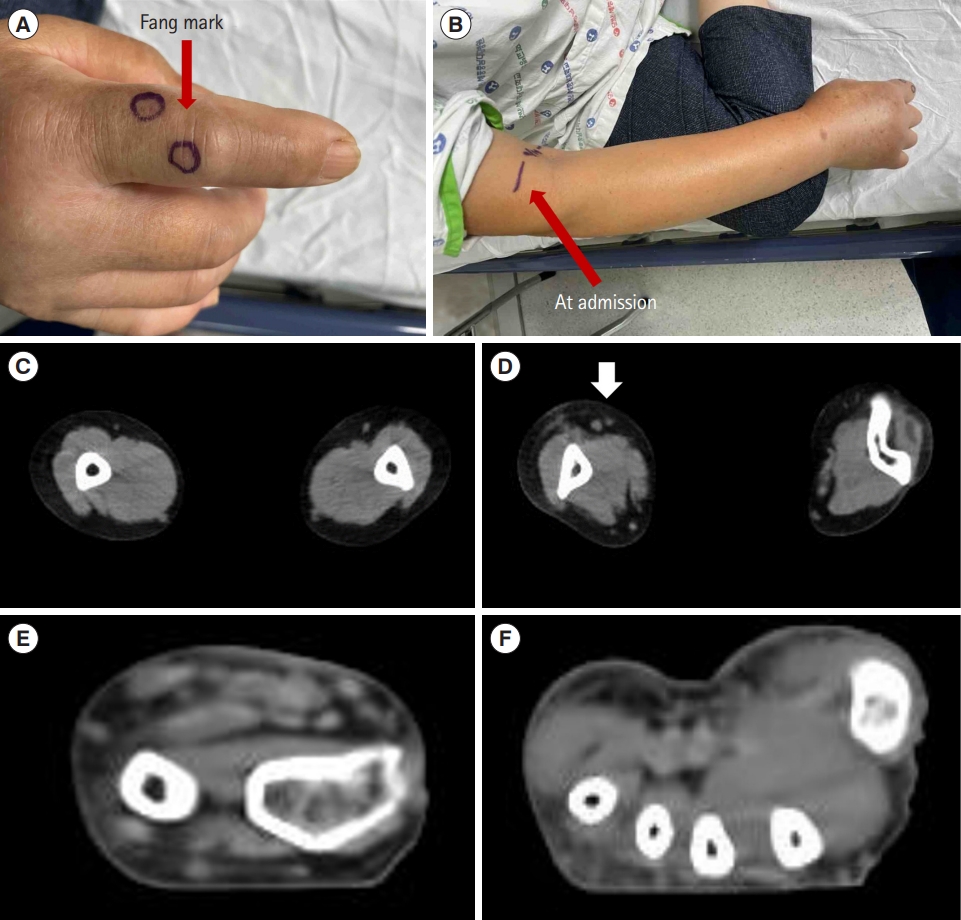
The second case was a 69-year-old woman with no past medical history admitted for a snakebite on her right second finger. She arrived at the emergency department of our hospital 45 minutes following the snakebite, with severe local pain and swelling that progressed to the distal humerus of the right arm. Making a fist was challenging due to the swelling (Fig. 2). The local effect score was 13 (pain, 4; swelling, 3; ecchymosis, 2; time, 4). The patient also complained of visual disturbances with diplopia and dizziness. However, there was no history of bleeding from the gums, epistaxis, hemoptysis, hematemesis, melena, vaginal bleeding, or loss of consciousness. Laboratory test results revealed no remarkable abnormalities (Table 1). A skin allergy test for antivenom administration was positive, and the patient was deemed unsuitable for antivenom administration. Therefore, pyridostigmine (Mestinon, Korean Drug) 180 mg/day (60 mg tablet three times daily) and VVse (Entelon) 300 mg/day (150 mg tablet twice daily) were administered to relieve the neurological symptoms and improve arm swelling, respectively [7,8]. The symptoms significantly improved on the third day following the snakebite. On the 5th day, the right arm swelling recovered to near normal, and the laboratory test results revealed no unusual findings (Table 1). The patient was discharged on the 5th day and continued VVse for an additional 6 days, for a total of 11 days. No specific findings were observed at the outpatient clinic 3 weeks following the snakebite.
The primary complaints of patients with snake bites are local symptoms of pain, swelling, and necrosis in the bite area. Generally, antivenoms do not provide sufficient protection against venom-induced local tissue damage [1ŌĆō6,9ŌĆō11].
Snake venom delivery typically occurs subcutaneously or can be intramuscular, releasing toxins into the interstitial space [3ŌĆō6]. Snake venom toxins interact with hyaluronic acid in the extracellular matrix, facilitating interstitial spread before entry into the vessels. This causes local damage to the vascular endothelium, resulting in local hemorrhage and edema and altered absorption characteristics of the damaged vessels. Viperid snake venoms are a rich source of metalloproteases. One of the most serious effects induced by metalloproteases is local hemorrhage including myonecrosis, blistering, coagulopathy, platelet effects, and proinflammatory activity.
From the interstitium, toxins diffuse through the extracellular matrix until they reach a vessel with a permeable endothelium, where they can be absorbed [3ŌĆō6,12,13]. The permeability of the blood vascular endothelium decreases as toxin molecular size increases. Large molecules are absorbed primarily through the lymphatics, producing a fundamentally different toxicokinetic profile from that of smaller toxins, which can achieve direct access to the blood capillaries [13]. Viperid snake venoms are rich in large molecule toxins and possess a pharmacokinetic profile characterized by a rapid initial absorption phase followed by a complex and slow absorption process from the site of venom injection [3ŌĆō6,12,13].
Viper bites produce more intense local reactions compared to other snakebites [1,2,6,10]. Swelling may become apparent within 15 minutes of the bite and becomes massive within 2 to 3 days, persisting for up to 3 weeks [12]. The swelling spreads rapidly from the site of the bite and may involve the entire limb and adjacent trunk owing to the action of hyaluronic acid and metalloproteases [11]. Regional lymphadenopathy may also develop as a result of the large molecule toxins and can hinder absorption of the retained fluid [10ŌĆō13]. If the envenomed tissue is contained in a tight fascial compartment, such as the pulp space of the digits or anterior tibial compartment, ischemia will develop [10ŌĆō13].
In case 1, the patientŌĆÖs leg swelling worsened rapidly, and ascites and lymphadenopathy were confirmed on APCT. However, antivenom alone did not improve these local symptoms. A treatment modality that could effectively control the local effects and ascites is warranted for use in such cases. In case 2, the patient exhibited an allergy to antivenom and presented with neurologic symptoms. Antivenom administration was contraindicated, and systemic symptoms, such as coagulopathy, were expected. Although the neurologic symptoms improved with pyridostigmine, control of the arm swelling was challenging. Similar to the first case, this shows the need for a treatment modality that can safely and effectively control toxic local effects.
In these cases, after a snakebite, one patient exhibited improvement within 7 days, and the other improved within 5 days. In previous studies in Korea and Japan, only the length of stay due to local swelling was investigated [14,15]. Since these patients were discharged from the hospital before complete symptom resolution, the exact period of improvement was unknown [14,15]. However, the length of stay was more than 2 weeks when the local effect score was 13 or higher and even longer when antivenom was not administered [14,15].
In studies on the effects of VVse on snake venom, Vitis vinifera extract has shown its ability to neutralize viper venom [3,5,6]. VVse effectively inhibited the caseinolytic, fibrinogenolytic, and hyaluronidase activities of the venom and efficiently neutralized its hemorrhage-inducing, edema-inducing, and myonecrotic properties. Moreover, the extract partially inhibited the procoagulant activity of the venom and inhibited degradation of the alpha and beta chains of human fibrinogen. Therefore, the extract possesses potent anti-snake venom properties, especially against the local effects of viper bites.
In conclusion, VVse may be able to treat the local toxic manifestations safely and effectively following a snakebite. Studies with larger sample sizes and studies determining the optimal initial dose of VVse for snake venom are warranted to further verify its efficacy.