Validation of the Korean criteria for trauma team activation
Article information

Abstract
Objective
We conducted a study to validate the effectiveness of the Korean criteria for trauma team activation (TTA) and compared its results with a two-tiered system.
Methods
This observational study was based on data from the Korean Trauma Data Bank. Within the study period, 1,628 trauma patients visited our emergency department, and 739 satisfied the criteria for TTA. The rates of overtriage and undertriage in the Korean one-tiered system were compared with the two-tiered system recommended by the American College of Surgery-Committee on Trauma.
Results
Most of the patient’s physiologic factors reflected trauma severity levels, but anatomical factors and mechanism of injury did not show consistent results. In addition, while the rate of overtriage (64.4%) was above the recommended range according to the Korean criteria, the rate of undertriage (4.0%) was within the recommended range. In the simulated two-tiered system, the rate of overtriage was reduced by 5.5%, while undertriage was increased by 1.8% compared to the Korean activation system.
Conclusion
The Korean criteria for TTA showed higher rates of overtriage and similar undertriage rates compared to the simulated two-tier system. Modification of the current criteria to a two-tier system with special considerations would be more effective for providing optimum patient care and medical resource utilization.
INTRODUCTION
Traumatic injury is a major cause of death in many countries [1-5]. It is important to consider that many young and productive people are included in trauma-related mortalities, which can have a negative effect on society and increase medical-care costs [6]. Therefore, many developed countries are trying to prevent severe trauma with social safety systems and reduce injury-related mortalities using specialized care systems for trauma patients. Implementing multidisciplinary care for trauma patients is one of the most well-known systems to increase the survival rate and reduce the disability rate [7-11]. This system requires the immediate assembly of the trauma team at the time of patient arrival at the emergency department (ED), so most trauma centers have a set of criteria for trauma team activation (TTA). The most important aspect of having such criteria for TTA is to minimize undertriage, to secure patient safety and minimize overtriage to prevent the overuse of medical resources [12-16]. The American College of Surgeons-Committee on Trauma (ACS-COT) recommends that the rate of undertriage should be less than 5% and overtriage less than 25% to 35% [17].
In South Korea, seven level I trauma centers have been in operation since 2011, and they have been using a common set of criteria for TTA (Table 1). These criteria are based on the ACS-COT field triage criteria for trauma patients, but unlike that criteria, any of the factors (physiological, anatomical and mechanism of injury) could be considered for activating the trauma team [7]. These newly modified criteria have never been evaluated for their effects on patient safety and appropriateness for application in our country. We conducted a study to validate the effectiveness of the Korean criteria for TTA and compared the results with a two-tiered system.
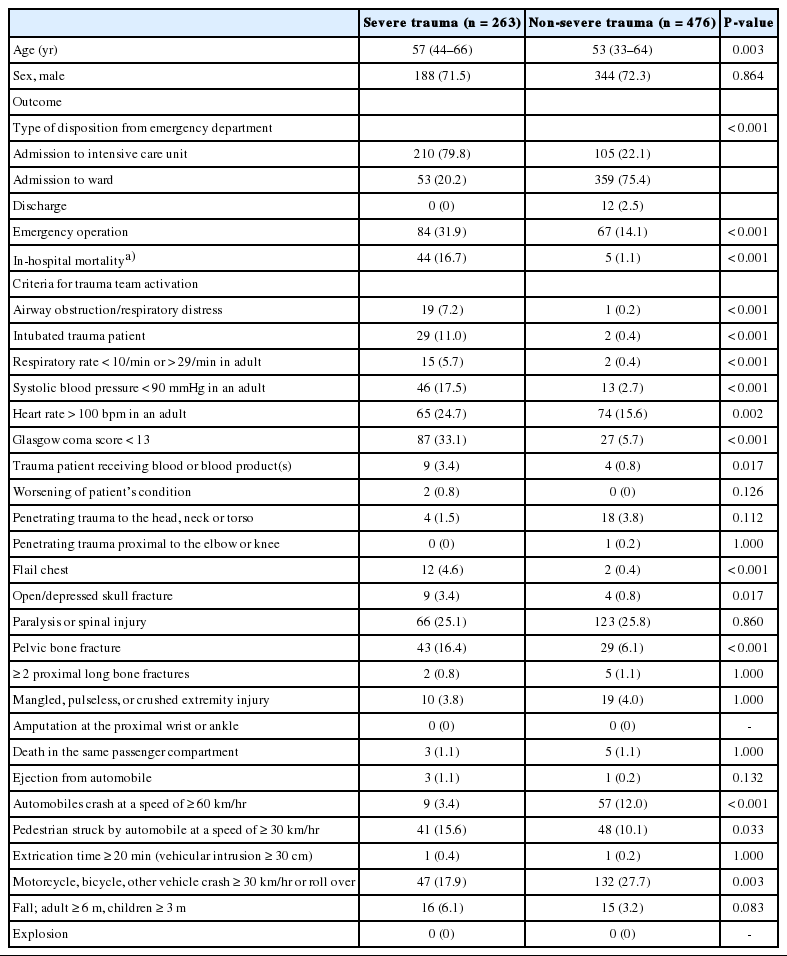
General characteristics and Korean criteria for trauma team activation in severe trauma (ISS>15) and non-severe trauma (ISS≤15) group
METHODS
Study design and hospital setting
This was a registry-based observational study of trauma patients who were admitted to the ED of a level I trauma center during the study period of June 2016 to November 2016. The study protocol was approved by the Institutional Review Board of Wonju Severance Christian Hospital where the research took place (CR317034) and informed consent was waived. In addition, this observational study was completed in accordance with the STROBE reporting guidelines for conducting original research.
Every year, more than 44,000 patients visit our ED, about 7% of whom are trauma patients. The trauma team consists of emergency physicians, general surgeons, thoracic surgeons, neurosurgeons, orthopedic surgeons, and anesthesiologists. When a patient satisfies the criteria for TTA, the emergency medicine board-certified physician (EP) on duty notifies the team via a short message service with relevant patient information including age, sex, mechanism of injury, and clinical impression. All assembled members of the trauma team then have to decide on the treatment plan for the patient, determine whether emergency surgery is needed, and assess whether admission to the intensive care unit (ICU) or general ward, transferring out, or discharge is required. All trauma patients can be managed in our trauma center, but those who need specialized burn care or emergency microsurgery of the hands or feet are usually transferred to another hospital.
Data sources
All trauma patients that visit or are referred to our hospital have been registered in the national trauma database, the Korean Trauma Data Bank. For these patients, information entered into the database includes patient characteristics, injury mechanism, injury severity, treatment modality and outcomes; age, gender, status of TTA, abbreviated injury scale score, injury severity score (ISS), blood pressure, heart rate, respiratory rate, Glasgow coma score (GCS), the type of ED disposition, ICU admission, and in-hospital mortality. In our hospital, variables in the Korean Trauma Data Bank have been collected by trauma center coordinators who oversee medical records at the time of patients discharge.
Validation and simulation of criteria for TTA
Severe trauma was defined as an ISS over 15 [18]. Correct triage was defined as severe trauma in a patient for whom the trauma team was activated or non-severe trauma in patients for whom the trauma team was not activated. Overtriage was defined as an ISS of 15 and below in a patient for whom the trauma team was activated. Undertriage was defined as an ISS above 15 in a patient for whom the trauma team was not activated [19]. Validation of each factor in the criteria for TTA was presented as an odds ratio (OR) of a correct triage compared with an overtriage or undertriage. Prehospital and in-hospital factors among patients classified as undertriaged were analyzed separately to ascertain the cause of the undertriage.
We performed overtriage and undertriage simulations for patients with physiological and anatomic factors associated with injury and trauma to compare the Korean single-tier TTA system with the ACS-COT recommendation, which is a two-tiered system used in many countries [13,15,20,21]. These criteria recommend that patients with anatomical or physiological factor(s) should be triaged to level I trauma centers while other patients should be triaged to the nearest trauma center regardless of the facility’s designated trauma level [7]. In South Korea, only the level I trauma centers were designated so that it might be reasonable to compare the accuracy of triage for the patients compatible to the level I trauma center. Therefore, we only included patients with physiological factor(s) or anatomical factor(s) from the data sources, as mentioned in the AST-COT recommendation, and calculated the rates of overtriage and undertriage in this simulation. We compared the rates of overtriage and undertriage between the original Korean criteria and the simulated two-tiered system criteria.
Evaluation of parameters related to undertriage
A history of anticoagulant medication use, bleeding disorders, open fractures, neurovascular compromise, end-stage renal disease and pregnancy >20 weeks of gestation were defined as “potentially serious injuries” according to the ACS-COT recommendation even though they were excluded in the Korean criteria for TTA [7]. Therefore, these variables were searched for in the medical records when a patient was classified as undertriaged and any of these factors were defined as the cause of undertriage.
Data analysis
Continuous data were presented as medians and interquartile ranges (IQRs) and compared using the Mann-Whitney U-test or the Kruskal-Wallis test as appropriate. Nominal data were presented as their frequencies of occurrence and compared using the chi-square or Fisher exact test as appropriate. Univariate analysis was performed to evaluate the association between each of the factors based on the Korean criteria for TTA and development of severe trauma. Multivariate logistic regression analysis was performed to verify factors related to the development of severe trauma. All variables with a two-sided P-value less than 0.05 in the univariate analysis were included in this analysis. The resulting ORs were presented together with their 95% confidence intervals (CIs) in univariate and multivariate analyses. The ORs with a CI above one and a two-sided P-value less than 0.05 were considered statistically significant. The Bonferroni correction method was used for the post hoc analysis after the Kruskal-Wallis test, and P-values less than 0.0167 were regarded as significant. All statistical analyses were performed using the PASW Statistics ver. 18.0 (SPSS, Chicago, IL, USA).
RESULTS
General characteristics
Within the study period, 1,628 trauma patients visited our ED, and 739 of them satisfied the criteria for TTA (Fig. 1). Two hundred and sixty-three patients were put into the severe trauma group and their median age was higher than the non-severe trauma group (P=0.003). There were more emergency operations, ICU admissions and in-hospital deaths in the severe trauma group (P<0.001, respectively); ward admission was more frequent in the non-severe group (P<0.001). The criteria for TTA and the difference between groups is shown in Table 1.
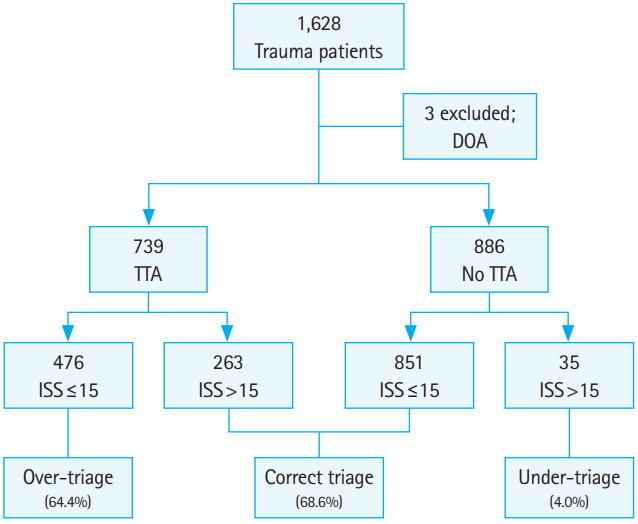
Study population and rates of triage. DOA, death on arrival; TTA, trauma team activation; ISS, injury severity score.
Validation of Korean criteria for TTA
In the univariate analysis, all the physiological factors except ‘worsening of patient’s condition’ were related to severe trauma. Flail chest, open/depressed skull fracture, and pelvic bone fractures were the anatomical factors related to severe trauma. Under the criteria for the mechanism of injury, ‘pedestrian struck by automobile at a speed of ≥30 km/hr’ and ‘motorcycle, bicycle, other vehicle crash ≥30 km/hr or roll over’ were inversely related to severe trauma. Automobile crashes at a speed of over 60 km/hr were inversely related to severe trauma (Table 2).

Univariate analysis of factors in Korean criteria for predicting severe trauma
Under the multivariate analysis, intubated trauma patients (OR, 6.901; 95% CI, 1.507 to 31.604; P=0.013), a systolic blood pressure below 90 mmHg (OR, 2.807; 95% CI, 1.340 to 5.880; P=0.006), a GCS below 13 (OR, 4.456; 95% CI, 2.611 to 7.607; P<0.001), flail chest (OR, 9.227; 95% CI, 1.926 to 44.198; P=0.005), and pelvic bone fracture (OR, 2.854; 95% CI, 1.660 to 4.909; P<0.001) were significantly associated with severe trauma. Automobile crash at a speed of 60 km/hr or over was inversely related to severe trauma (OR, 0.421; 95% CI, 0.202 to 0.878; P=0.021) (Table 3).

Multivariate analysis of factors in Korean criteria for predicting severe trauma
The rate of correct triage was 68.6% for the Korean criteria even though the rates of overtriage and undertriage were 64.4% and 4.0%, respectively (Fig. 1). The median age was lowest in the overtriaged group (P=0.006) even though there was no significant difference in terms of gender (P=0.675). The ISS, the frequency of emergency operations and the rate of ICU admission were lowest in the overtriaged group (P<0.001). The in-hospital mortality rate was highest in the correctly triaged group (P<0.001) (Table 4).
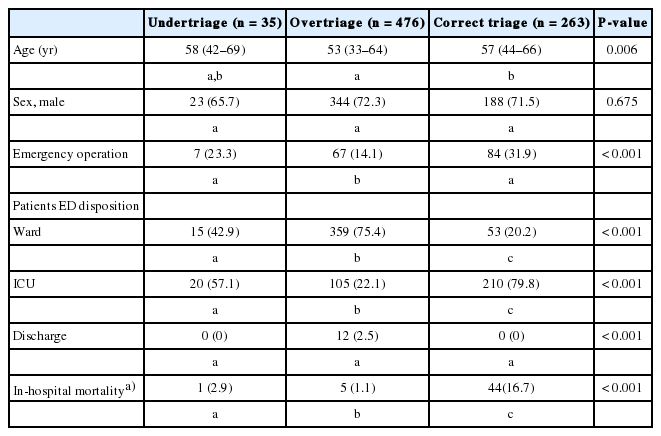
Comparison of triage groups by current trauma team activation
A total of 35 patients were classified as the undertriaged group. Twenty-three patients (65.7%) were male and the median ISS was 17 (IQR, 16 to 23). Twenty-one patients (60%) were transferred from other hospitals after stabilization and the diagnostic process and their mean elapsed time from injury to presentation at our hospital was 31.3±86.5 hours. The types of injuries included the following: single body part (n=10, 28.6%), head injuries (n=5, 14.3%), thoracic injury (n=1, 2.9%), abdominal injury (n=1, 2.9%), spinal injury (n=1, 2.9%), pelvic injury (n=1, 2.9%) and hanging (n=1, 2.9%). These patients were assessed and referred to the appropriate departments. Two patients (5.7%) were on anticoagulant medication, and two others (5.7%) were classified as decision errors by the EP on duty.
Simulation of two-tiered system for TTA
In the simulated two-tiered system, the rate of overtriage was reduced by 5.5%, and the rate of undertriage was increased by 1.8% compared to the Korean activation system. However the frequencies of ICU admission, emergency operation, and in-hospital mortality were similar in the two groups (Table 5).

Comparison of two models simulation for trauma team activation
Patients excluded from the simulation had a lower median ISS of 9 (IQR, 5 to 14), a lower frequency of ICU admission (21.6%) and emergency operations (10.5%) than patients in the two-tiered system. There was no in-hospital mortality in this group.
DISCUSSION
In the Korean criteria for TTA, physiological factors were promising criteria for anticipating severe trauma, but anatomical factors, mechanism of injury and the discretion of the attending EP did not show consistent results. Since most physiological factors objectively represent the patient’s condition and can be defined clearly and easily, there is little chance of misunderstanding the patient’s status or hesitating decisions when implementing TTA [22-25]. On the other hand, since the anatomical factors and mechanisms of injury are more subjective, it is difficult to judge whether each factor corresponds correctly within a short time because it is hard to determine the severity of injury with anatomical factors based solely on the physical examination. It is also challenging to deduce the exact mechanism of injury through history taking from patients or from emergency medical technicians. The establishment of social safety systems, such as the generalization of automobile safety systems, the obligation of fastening seat belts, and the mandatory safety management of workplaces may have changed the previously established relationship between the mechanism of injury and the severity of trauma [26-28]. The inverse relationship between automobiles crashing at a speed of 60 km/hr or over and severe trauma in this study might be an example of this consideration. Therefore, newly modified criteria based on recent trauma databases are needed to promote the predictability of criteria for TTA.
Using the Korean criteria for the analysis showed a rate of overtriage above the recommended range even though the rate of undertriage was within the recommended range [17]. These results were affected by strictly defined physiological factors such as heart rate, respiratory rate, and GCS, which differed from the criteria of other countries [29-32]. Physiological factors are very sensitive, but not specific, for identifying patients with severe trauma so overtriage would evidently be increased and undertriage would be decreased [33]. This could be another reason for the high rate of overtriage since triage is performed first in the ED, not on the field, unlike other countries [34].
The simulated validation, excluding mechanisms of injury only, showed a lower rate of overtriage and a higher rate of undertriage compared to results from the original Korean criteria. Minimizing overtriage is essential for reducing overuse of medical resources, but minimizing undertriage is more important for ensuring a patient’s safety [35,36]. Therefore, assembling physicians and surgeons with a single-tier TTA system rather than in a systematic fashion would be better for caring for patients with severe trauma. However, it would be inefficient to assemble the entire trauma team, regardless of the severity of the patient’s condition. Some countries have used a two-tier system for TTA to promote patient safety and reduce the inefficient use of medical resources [15,16,20]. They have separate options which may include activating the entire trauma team or only some physicians and surgeons as first responders depending on the severity of the patient’s condition [15,16,20,21,32]. We could apply this ‘reduced TTA’ for patients with certain kinds of mechanisms of injury only. In our study, a patient’s condition with respect to the mechanism of injury only showed a lower ISS and a lower frequency of ICU admission and emergency operation when compared to the other patients and there was no in-hospital mortality. Reduced TTA might minimize medical resource overuse and the rate of undertriage in this situation.
Many undertriaged patients were transferred to our trauma center after 24 hours following the injury in our study. Inter-hospital transfer after stabilization and the diagnostic process were the major factors associated with the long transport time in these patients. In these cases, the physician or surgeon responsible for the patient’s care might be decided upon arrival at the ED. For this reason, the entire trauma team may not need to be activated in this situation. In some other countries’ criteria, special considerations for the possible overuse of medical resources are defined separately. For example, they only include patients who visit the ED within 24 hours after injury [20,30]. Furthermore, patients with a high probability of deterioration, such as those on anticoagulant medication, those with bleeding disorders and liver cirrhosis are given special consideration [7,20,29]. It was also noticed that patients on anticoagulant medication were undertriaged in our study. Adding these special considerations as reference details to the criteria of the attending EP’s discretion and the criteria for reduced TTA would effectively modify the current Korean criteria for TTA.
This study has several limitations. First, this was a single-center observational study even though a relatively large sample size was used. We expect that validation and modification of the Korean criteria for TTA, based on the national trauma database, will be performed to ensure its predictability and effectiveness in the near future. Second, the mechanism of injury might be entered incorrectly depending on the judgment of the inputter even though we used a coding system to minimize interpersonal variation. Third, personal variations in the accuracy of each EP’s clinical judgment could affect the rates of overtriage and undertriage. Fourth, it is hard to interpret the cause of an inverse relationship between high speed automobile accidents and severe trauma because information about safety systems (e.g., seat belt use in automobile accidents or helmet use in motorcycle accidents) was not securely collected in our registry.
In conclusion, the Korean criteria for TTA showed a higher rate of overtriage than the recommended range even though the rate of undertriage was within the recommended range. The lower overtriage and similar undertriage rates than current Korean criteria were noticed in simulated two-tiered system. Modification of the current criteria to a two-tier system with addition of special considerations that facilitate an emergency physician’s decision would be more effective for providing optimum patient care and medical resource utilization.
Notes
No potential conflict of interest relevant to this article was reported.
References
Article information Continued
Notes
Capsule Summary
What is already known
Multidisciplinary care for trauma patients is the best way to increase the survival rate and reduce the disability rate and trauma team activation (TTA) is the starting line for its success. Developed countries have validated and modified the criteria for TTA for securing patient safety and minimizing overuse of medical resources.
What is new in the current study
Korean criteria for TTA showed lower overtriage rates and similar undertriage rates compared with those of other countries. Modification of the current criteria to a two-tier system with special considerations would be more effective for providing optimum patient care and medical resource utilization.