Comparison of trauma systems in Asian countries: a cross-sectional study
Article information

Abstract
Objective
This study aimed to compare the demographic characteristics and trauma service structures and processes of hospitals in 15 countries across the Asia Pacific, and to provide baseline data for the integrated trauma database: the Pan-Asian Trauma Outcomes Study (PATOS).
Methods
Medical directors and emergency physicians at PATOS-participating hospitals in countries across the Asia Pacific were surveyed through a standardized questionnaire. General information, trauma care system data, and trauma emergency department (ED) outcomes at each hospital were collected by email and analyzed using descriptive statistics.
Results
Survey data from 35 hospitals across 15 countries were collected from archived data between June 2014 and July 2015. Designated trauma centers were identified as the highest hospital level for trauma patients in 70% of surveyed countries. Half of the hospitals surveyed had special teams for trauma care, and almost all prepared activation protocol documents for these teams. Most hospitals offered specialized trauma education programs, and 72.7% of hospitals had a hospital-based trauma registry. The total number of trauma patients visiting the ED across 25 of the hospitals was 300,376. The overall survival-to-discharge rate was 97.2%; however, it varied greatly between 85.1% and 99.7%. The difference between survival-to-discharge rates of moderate and severe injury groups was highest in Taiwan (41.8%) and lowest in Thailand (18.6%).
Conclusion
Trauma care systems and ED outcomes vary widely among surveyed hospitals and countries. This information is useful to build further detailed, systematic platforms for trauma surveillance and evidence-based trauma care policies.
INTRODUCTION
The World Health Organization (WHO) reported that injuries cause more than 5 million deaths worldwide each year, and injury mortality is expected to surge by 2030 [1]. Injury is one of the leading causes of death during the productive years (<45 years old), leading to significant economic losses [1]. In addition, injury accounts for 8.3% of age-standardized disability-adjusted life years (DALYs), with road traffic injuries ranked 8th out of the 20 leading causes of DALYs in 2012 [2].
However, the burden of injury differs by region. One of every ten deaths in Asia is attributed to injury, accounting for more than half of injury-related deaths worldwide [3]. According to the WHO, injuries were responsible for 87,583 of DALYs per 100,000 people in Southeast Asia in 2012; far more than the 38,903 of DALYs per 100,000 people in high-income countries. Even among Asian countries, there is a large discrepancy. Injury mortality rates vary greatly from 20.6 deaths per 100,000 people in Singapore, to 346.6 per 100,000 people in Myanmar [4]. Rapid economic development and urbanization are considered contributing factors for the increase in injury-related death and disability in developing countries of this region [3].
To reduce the burden of injury, a well-functioning trauma care system is essential. The WHO published “Guidelines for essential trauma care” through the Essential Trauma Care Project, and emphasized the importance of establishing trauma care systems to improve trauma treatment, and hence, patient outcomes. Panel studies reported a 50% average reduction in preventable death rates after the implementation of a trauma system [5], and other studies demonstrated a morbidity and mortality decrease with organized optimal trauma care [6-8]. The effectiveness of trauma system development has been proven for each component of prehospital, hospital and inter-hospital systems for trauma care [5,7,9-11].
Most Asian countries recognize their increasing injury burden and have made efforts to build qualified trauma care systems [12-16]. However, these efforts have met with varied success because of unequal healthcare resources and resource allocation, along with socioeconomic, cultural, and demographic variance [12-16]. A comprehensive report-based trauma database for Asian countries is required, to identify trauma characteristics in different contexts, monitor discrete trauma systems, and generate evidence-based trauma care policies.
The Pan-Asian Trauma Outcomes Study (PATOS) is an international, multicenter, population-based, cohort study in the Asia Pacific region, proposed in 2013 to create an integrated trauma database. PATOS will collect standardized data on diverse trauma epidemiology, trauma care processes, and outcomes from participating hospital emergency departments across 15 Asian countries for the next 3 years. The objectives of this web-based, cross-sectional, descriptive survey were to examine and compare the demographic characteristics and trauma care service structures, processes and outcomes of trauma care services of PATOS-participating hospitals. Moreover, this study will provide baseline data for PATOS.
METHODS
Study design and setting
The study protocol was approved by the institutional review board of Seoul National University College of Medicine (H-1509-045-702). This cross-sectional survey was conducted among medical directors and emergency physicians in the emergency medical services (EMSs) and trauma care systems at PATOS-participating hospitals in 15 Asia Pacific countries: Australia, China, Hong Kong, India, Indonesia, Japan, Malaysia, Myanmar, Philippines, South Korea, Singapore, Taiwan, Thailand, Uzbekistan, and Vietnam.
These 15 countries have varied population characteristics and health indices (Table 1) [17-20]. A wide variation in economic status has been observed regarding gross domestic product per capita: five countries have less than $10,000/capita, four countries have between $10,000 and $30,000/capita, and six countries have more than $30,000/capita. Health indicators also vary within medical settings. The burden of injury is considerable in India and Myanmar, where more than 100 people die from injuries per 100,000 people, and almost 4,800 years of life lost (YLL) per 100,000 people are attributed to injuries. Developed countries, such as Australia, Singapore, and Japan have low injury mortality rates and YLL. Extraordinarily, the injury mortality in South Korea is 53 deaths per 100,000 people, which is 44% higher than the average injury mortality rate of high-income countries. In addition, injury-associated YLL is higher in South Korea, with 2,381 YLLs per 100,000 people, compared to an average of 2,142 per 100,000 people in high-income countries [17].

Population characteristics and health indices
Study participants
Survey respondents were trauma surgeons, emergency physicians, general surgeons, and public health, EMS, and hospital officials at PATOS-participating hospitals and EMS systems. Only one survey was permitted per hospital.
Data collection and protocols
Data were collected from June 2014 to August 2015, through the standardized survey form developed and revised by a team of emergency physicians at the PATOS coordinating center in South Korea. The survey form was sent to every individual on the PATOS mailing list, who submitted their responses to the PATOS coordinating center by e-mail. The hospital survey (Appendix 1) comprised seven questions regarding general hospital information, eight questions on trauma care processes, five questions on trauma education programs, six questions on trauma registries, and twelve questions on trauma outcomes. The PATOS committee validated the survey results and communicated with respondents when errors were found.
Measurements
General hospital information, such as a country and hospital name, the number of total visits to the ED, and trauma center or hospital level was collected. Urbanization of the community to which the responding hospital belonged was categorized as urban, suburban, rural, or wilderness. We defined “urban” as a city with more than 2,500 inhabitants/km2 and “rural” with fewer than 2,500 inhabitants/km2. However, respondents could choose multiple answers from urban, suburban, rural, or wilderness according to their own definition. Trauma center level was categorized as a designated trauma center, a general ED, or a general hospital. Hospital level was classified as tertiary, secondary, or primary care according to their definition.
The trauma care process was identified from the answers to specific questions, such as “Who takes responsibility for the trauma care? Is it a trauma surgeon, emergency physician, general surgeon, or another department surgeon?” and “Which hospital level is the highest for trauma patients?” In addition, we collected detailed information regarding trauma resources, including trauma teams, trauma surgeons, and trauma centers.
If present, trauma structures, trauma education programs, and registries were described by respondents, who clarified whether their trauma education programs were mandatory, and if the program included operation and critical care practices. Respondents were also asked whether hospital registries were linked to prehospital registries.
ED outcomes included the total number of ED visits, trauma patients’ survival-to-discharge rate, and proportion of EMS users among trauma patients. Trauma severity was assessed using the injury severity score (ISS) index: 9–15, 16–24, and >24.
Statistical analysis
All survey responses were entered into Microsoft Excel (Redmond, WA, USA), and analyzed using descriptive statistics. Although data were collected from individual hospitals, they were compared by country. Trauma care outcomes were only partially reported because of lack of the available information from some hospitals.
RESULTS
Characteristics of participating hospitals
PATOS members from thirty-five hospitals received the survey and responded by June 2014 (response rate, 100%). The total number of ED visits to these hospitals at the time of the survey was 2 million per year, and average visits per hospital was approximately 71,000. Singapore had the largest number of ED patients per hospital (154,541 visits), and Uzbekistan had the smallest (15,000 visits). Three-quarters of surveyed hospitals were located in urban areas. Twenty-six percent of hospitals (n=9) were designated trauma centers, and others were general hospitals with EDs. The majority of participating hospitals were tertiary care hospitals (77%, n=27). Table 2 details the general characteristics of participating hospitals.
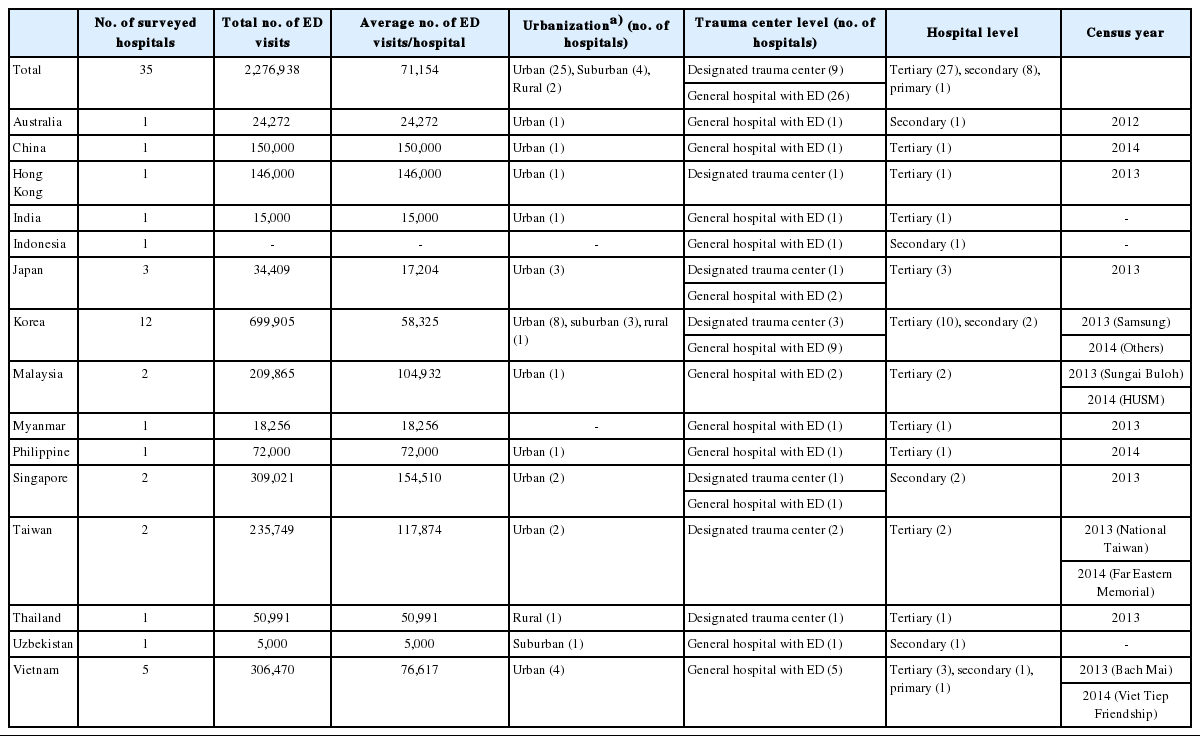
General hospital information of surveyed hospitals
Trauma care system: process
Seventy-two percent of respondents indicated that designated trauma centers were at the highest hospital level for trauma patients, yet respondents in Indonesia, Malaysia, and Uzbekistan all reported that general hospitals with EDs were at the highest hospital level for trauma care. Half of the hospitals in this survey had designated teams for trauma care, and most were prepared with trauma team activation protocols. Australia, Japan, and Indonesia did not have trauma teams, but respondents indicated that documented trauma protocols existed. Trauma care services were provided by emergency physicians and trauma surgeons in 60% of the surveyed hospitals. Ten countries issued a specific trauma surgeon certification or license. Table 3 details the trauma care process of surveyed hospitals.

Trauma care process of surveyed hospitals
Trauma care system: structure
Most hospitals offered specialized trauma education programs for medical staff (91%, n=30) However, only one-third of programs were mandatory. Hospital-based registries for trauma were used at 72.7% of hospitals. Trauma registries in Hong Kong, Japan, Korea, Malaysia, Singapore, Taiwan, and Uzbekistan contained prehospital information, such as intubation treatment, and some of these registries were even more comprehensive as they were connected to an EMS-based registry. Systematic review programs for trauma care existed in approximately half of the hospitals (53.8%). Table 4 details the trauma care system of surveyed hospitals [17].

Trauma care structure of surveyed hospitals
Trauma outcomes
Patient data were available for 25 of the 35 EDs. The total number of trauma patients across these sites was 300,376. Eleven (45.6%) of these hospitals, located in Japan, Korea, Philippines, Singapore, and Thailand, reported outcomes for ED trauma patients. The overall survival-to-discharge rate in these hospitals was 97.2%, and rates varied from 85.1% (Taiwan) to 99.7% (Singapore). The outcomes of trauma patients using EMS were reported in 10 of these hospitals, and these patients tended to have a worse outcome compared to trauma patients in general (survival-to-discharge rate 94.7% vs. 97.2%, respectively). The average survival-to-discharge rate was 96.3% in patients with an ISS of 9 to 15, and 65.1% in patients with an ISS of >24. The difference between survival-to-discharge rate of patients with an ISS of 9 to 15 and patients with an ISS of >24 was highest in Taiwan (41.8%) and lowest in Thailand (18.6%). Table 5 details trauma outcomes among surveyed hospitals.

Trauma ED outcomes of surveyed hospitals
DISCUSSION
We collected and described survey data regarding sociodemographic characteristics, trauma care processes, trauma care structures including education programs and registries, and ED trauma outcomes from 35 individual hospitals across 15 Asia Pacific countries. Our findings showed a wide variety of trauma care systems and outcomes among countries.
Specific trauma care education for medical staff is an essential component of adequate trauma care [14,21,22]. For example, the Japan Advanced Trauma Evaluation and Care education program significantly reduced trauma mortality [22]. Most hospitals in our study had established trauma-specialized education programs, but 60% of them were not mandatory, and education programs for paramedics were insufficient. The shortage of standardized and organized educational programs for trauma care in Asian countries has also been reported by other studies [14,21,22].
Injury surveillance guidelines [23], published by the WHO in 2001, strongly recommended injury surveillance systems with qualified, extensive injury data. The American College of Surgeons also emphasizes the importance of trauma registries for evaluating trauma systems [24]. We expect the PATOS to function in a similar way to the National Trauma Data Bank of the United States [25], National Trauma Registry of Canada [26], Trauma Registry of the German Society for Trauma Surgery [27], and EuroTARN—the Collaborative European Registry of Trauma of 14 European countries [28], by serving as a platform for analyzing trauma indices, comparing trauma care systems, and examining various risk factors and predictors of trauma in this region. We found that some hospitals in Hong Kong, Malaysia, Singapore, and Korea had linked registries for prehospital and hospital data, but others lacked this resource. PATOS will provide a reference to compare the benefits of resources like these to trauma outcomes across the Asia Pacific.
In our study, 75% of participating hospitals offered tertiary care, but only 25% had designated trauma centers. In Indonesia, Malaysia, and Uzbekistan, the highest hospital level for trauma patients was a general hospital, not designated as a trauma center; however, some hospitals in these countries were equipped with trauma teams. Designated trauma centers have been shown to improve survival and cost-effectiveness in several studies [11,29]. The United States has more than 1,000 trauma centers and manages the quality of services through American College of Surgeons certification [30]. India has established the Jai Prakash Narayan Apex Trauma Center at the All India Institute of Medical Sciences in New Delhi [10], and in South Korea, regional trauma centers have been designated and are currently being built [31]. In Australia, the introduction of a statewide trauma system was associated with significant improvements in trauma care outcomes [32].
It was not possible to collect ED trauma outcome data from some of the countries in this study. This may be attributed to the lack of trauma registries. One previous study reported that the mortality rate of injuries (ISS ≥9) rose from 35% in high-income settings to 63% in low-income settings [33], and a similar study showed that moderate injuries were associated with a 6% mortality rate in high-income countries, and a much higher 36% mortality rate in low-income countries [34]. In the current study, it is notable that survival-to-discharge rates for total trauma patients and trauma patients transferred using the EMS in Taiwan were both lower (85.1% and 72.2%, respectively) compared to other developed countries, and survival-to-discharge rates from moderate-to-severe trauma in South Korea did not meet the average. A previous study found trauma care outcomes in Japan to be unfavorable; the preventable death rate in Japan was 11% [13] compared to between 1% and 7% in the United States [35,36].
One limitation of this study was the small number of respondents for trauma outcomes (total ED survival [n=11] and survival rate by ISS [n=9]), which reduces the impact of comparisons between components of trauma care and mortality. Another limitation was lack of representation; our study generally included one to three hospitals per country, apart from the 11 hospitals in South Korea and the five hospitals in Vietnam. This potential selection bias makes it difficult to generalize our results, leaving us with only a partial understanding of the overall state of trauma care systems in each country. Moreover, we need to be careful when interpreting the results of this study because of profound discrepancies in the definitions of variables, and data quality. For example, standards for a designated trauma center could be different between countries, and the curriculum of education programs for trauma care could be more or less comprehensive in different countries. Some countries provided estimates rather than predefined and measured data, and exact data was often not available because trauma registries were not yet organized sufficiently. Missing or roughly estimated data for several variables, particularly trauma treatment outcomes, limited a robust description and comparison.
Our findings emphasize the differences in trauma ED outcomes across Asian trauma care settings, and support the need for a detailed, customized, and systematic trauma surveillance platform like PATOS. This study provides evidence-based data for the construction of organized trauma care systems based on a comprehensive trauma database, thereby helping to improve trauma outcomes in this region.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This paper was supported by Wonkwang University in 2018.
References
Appendices
Appendix 1. Hospital based survey form
ceem-18-088-app.pdfArticle information Continued
Notes
Capsule Summary
What is already known
Most Asian countries recognized their increasing injury burden and have put forth efforts to build qualified trauma care systems.
What is new in the current study
Half of the hospitals had organized special teams for trauma care and almost all of these prepared activation protocol documents for their teams. Most hospitals offered specialized trauma education programs, and 72.7% of hospitals had a hospital-based trauma registry. The overall survival discharge rate was 97.2%, however, varied greatly between 85.1% and 99.7%. A survival difference between moderate and severe injury groups was highest in Taiwan (41.8%) and lowest in Thailand (18.6%).