Reduced-Dose Systemic Fibrinolysis in Massive Pulmonary Embolism: A Pilot Study
Article information

Abstract
Objective
Severe pulmonary embolism (PE) has a high mortality rate, which can be lowered by thrombolytic therapy (TT). However, full-dose TT is associated with major complications, including life-threatening bleeding. The aim of this study was to explore the efficacy and safety of extended, low-dose administration of tissue plasminogen activator (tPA) on in-hospital mortality and outcomes in massive PE.
Methods
This was a single-center, prospective cohort trial at a tertiary university hospital. A total of 37 consecutive patients with massive PE were included. A peripheral intravenous infusion was used to administer 25 mg of tPA over 6 hours. The primary endpoints were in-hospital mortality, major complications, pulmonary hypertension, and right ventricular dysfunction. The secondary endpoints were 6-month mortality and pulmonary hypertension and right ventricular dysfunction 6 months after the PE.
Results
The mean age of the patients was 68.76±14.54 years. The mean pulmonary artery systolic pressure (PASP; 56.51±7.34 mmHg vs. 34.16±2.81 mmHg, P<0.001) and right/left ventricle diameter (1.37±0.12 vs. 0.99±0.12, P<0.001) decreased significantly after TT. Tricuspid annular plane systolic excursion (1.43±0.33 cm vs. 2.07±0.27 cm, P<0.001), myocardial performance index (0.47±0.08 vs. 0.55±0.07, P<0.001), and systolic wave prime (9.6±2.8 vs. 15.3±2.6) increased significantly after TT. No major bleeding or stroke was observed. There was one in-hospital death and two additional deaths within 6 months. No cases of pulmonary hypertension were identified during follow-up.
Conclusion
The results of this pilot study suggest that an extended infusion of low-dose tPA is a safe and effective therapy in patients with massive PE. This protocol was also effective in decreasing PASP and restoring right ventricular function.
Trial registration
ClinicalTrials.gov identifier: NCT02029456
INTRODUCTION
Pulmonary embolism (PE) is a life-threatening disease requiring early diagnosis and treatment. Thrombolytic therapy (TT) is often required in patients with massive PE [1]. Severe PE has a high mortality rate, and the in-hospital all-cause case mortality rates among unstable patients who receive TT are lower than among those who do not [1]. However, only a minority (≤30%) of unstable patients actually receive TT [2,3] for reasons that remain unclear. The high rate of complications associated with TT, including life-threatening bleeding, and insufficient data from the massive PE population might explain the reluctance to use TT.
The lungs are the only organ to receive the entire cardiac output, which makes them the point of convergence for all of an administered thrombolytic agent, independent of the route of administration. Therefore, lowering the dose of TT might both maintain its effectiveness in patients with massive PE and enhance its safety profile. Percutaneous endovascular interventions for deep venous thrombosis have suggested that low-dose thrombolysis can induce a favorable pulmonary response [4]. The aim of the present pilot study was to explore the efficacy and safety of an extended administration (6 hours) of low-dose (25 mg) tissue plasminogen activator (tPA) in patients with massive PE.
METHODS
Ethics statement
This study was approved by the Institutional Review Board of the University of Health Sciences Ahi Evren Chest Cardiovascular Surgery Education and Research Hospital (No. 2014-02029456), and patients were enrolled after providing informed consent. This study conforms with the principles of the Helsinki declaration and is registered in ClinicalTrials.gov ((identifier: NCT02029456).
Patient population and enrollment
This single-center, prospective observational pilot study explored the effectiveness of an extended administration of low-dose TT in treating massive PE. We hypothesized that the most serious complication of TT (bleeding) could be diagnosed early, and that a slow, low-dose TT infusion could be stopped immediately. We did not use concomitant heparin anticoagulation with TT due to the potential increased risk of bleeding.
Between May 2011 and May 2014, we enrolled 37 consecutive patients aged 18 years or older with confirmed massive PE (Fig. 1). PE was defined according to current guidelines as patients presenting with signs and symptoms suggestive of PE plus imaging documentation of PE on computed-tomographic angiography [1]. Massive PE was defined as acute PE with sustained hypotension (systolic blood pressure <90 mmHg for at least 15 minutes or a need for inotropic support that was not due to a cause other than PE, such as arrhythmia, hypovolemia, sepsis, or left ventricular [LV] dysfunction), pulselessness, or persistent profound bradycardia (heart rate <40 beats/min with signs or symptoms of shock). Patients with a prior intracranial hemorrhage, known structural intracranial cerebrovascular disease (e.g., arteriovenous malformation), known malignant intracranial neoplasm, ischemic stroke within 3 months, suspected aortic dissection, active bleeding or bleeding diathesis, recent surgery encroaching on the spinal canal or brain, or recent significant closed-head or facial trauma with radiographic evidence of bony fracture or brain injury were excluded from the study. The patient demographic characteristics, medical history, rhythm disorders, New York Heart Association (NYHA) classification, and primary symptoms were prospectively entered into a database.

Study flowchart.
Echocardiography
Each patient underwent a transthoracic echocardiographic evaluation before the TT, within an hour after the TT, before discharge (5–7 days), and a month after the TT. Pulmonary artery systolic pressure (PASP) was estimated from the tricuspid valve regurgitant jet velocity using the modified Bernoulli equation: 4v2+right atrial pressure [5]. The maximum dimensions of the right/left atria were measured in the standard four-chamber view. The diameter and collapsibility of the Inferior vena cava were noted. Pulmonary hypertension was defined as a PASP of >40 mmHg. Right ventricular (RV) enlargement was defined as an RV/LV ratio of >0.9. Tricuspid annular plane systolic excursion (TAPSE), tissue-Doppler– derived tricuspid annular systolic velocity, and the myocardial performance index (MPI), or Tei index, were recorded.
Computed tomography
All patients underwent 64-slice computed-tomographic pulmonary angiography (Aquilion 64, Toshiba Medical Systems) upon admission to the hospital to definitively diagnose PE. Patients underwent additional computed-tomographic angiography 24 hours after the completion of TT if their estimated glomerular filtration rate was >60 mL/min/1.73 m2 according to the modified diet in renal disease formula.
Thrombolytic therapy
After the diagnosis of massive PE, a 6-hour intravenous infusion of 25 mg of tPA without a bolus was administered immediately. If hemodynamic instability persisted despite the first dose of TT, a second 6-hour infusion of 25 mg of tPA without a bolus was administered. Anticoagulation with intravenous unfractionated heparin was withheld during thrombolytic agent infusion. Heparin, administered as a 70-U/kg bolus followed by a 1,000-U/hr infusion with a target activated partial thromboplastin time between 1.5 and 2.5 times the control was started immediately after the infusion of thrombolytic agent. After successful thrombolysis, warfarin was restarted while the patient was still on intravenous heparin.
Criteria for thrombolytic success
The following are the criteria for thrombolytic success: (1) Doppler documentation of the resolution of high PASP (<40 mmHg); (2) decreased right ventricular diameter (at least 25% decrease of RV/LV diameter); (3) restoration of RV function (TAPSE >16 mm); (4) systolic wave prime (S’) >10.0 cm/sec; (5) tissue-Doppler–derived RV MPI >0.55; and (6) clinical improvement of symptoms and restoration of stable hemodynamic status immediately after TT. Complete success was defined as clinical improvement of symptoms and restoration of stable hemodynamic status with at least three of the other criteria and without resultant death or nonfatal major complications.
The primary endpoints in this study were in-hospital mortality, nonfatal major complications, the development of pulmonary hypertension, and RV dysfunction. The secondary endpoints were 6-month mortality and pulmonary hypertension and RV dysfunction at 6 months.
Definition of complications
The definitions of complications used are the following: (1) inhospital mortality; (2) nonfatal major complications (ischemic stroke, intracranial hemorrhage, embolism [coronary or peripheral], bleeding requiring transfusion); and (3) nonfatal minor complications (bleeding not requiring transfusion [bleeding resulting in a hemoglobin drop <3 g/dL]).
Statistical analysis
Analyses were conducted using SPSS ver. 17.0 (SPSS Inc). Continuous variables are expressed as the mean±standard deviation for parameters with a normal distribution or median (interquartile range) for parameters with a non-normal distribution. Categorical variables are expressed as percentages. The analysis of normality was performed with the Kolmogorov-Smirnov test. Repeatedmeasure analysis of variance testing was used to analyze the dependent variables. The Bonferroni test was used as a post hoc analysis to adjust for multiple comparisons. A two-sided P<0.05 was considered significant.
RESULTS
This trial enrolled 37 consecutive patients (15 male patients) with massive PE. The mean age of the patients was 68.76±14.54 years, and 22 patients (59.5%) were older than 70 years. The baseline clinical characteristics of the patients are presented in Table 1. Twenty-two patients (59.5%) had hypertension, seven patients (18.9%) had diabetes mellitus, 12 patients (32.4%) had chronic obstructive pulmonary disease, eight patients (21.6%) had coronary artery disease, and five patients (13.5%) had congestive heart failure. Seventeen patients (45.9%) had accompanying deep venous thrombosis. All patients were followed for 6 months. The most common symptoms on admission were dyspnea and palpitations (Table 1). All the patients were hypotensive, and their mean systolic and diastolic blood pressures at admission were 76.19±8.52 and 49.62±7.82 mmHg, respectively. Blood pressure recovered within a few hours after the initiation of TT in all cases. The median troponin values (0.4 ng/mL; interquartile range, 0.30–0.76 ng/mL) were elevated at hospital admission. The mean length of hospital stay was 6.1±1.07 days (Table 2). Of the 37 patients, 18 (48.6%) underwent repeat pulmonary computed tomography angiography 24 hours after TT. Of those 18 patients, total lysis of the thrombus was observed in 16 patients (88.9%), and the remaining two patients had >75% lysis of the thrombus.
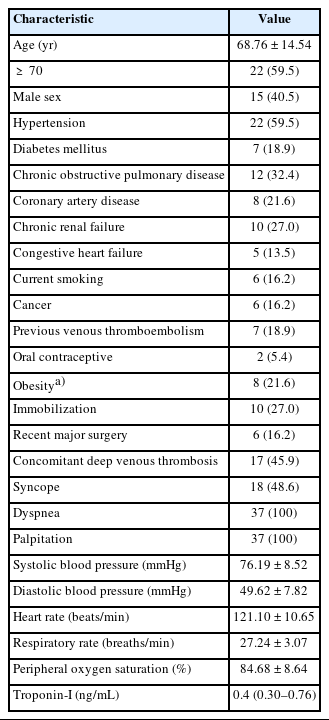
Baseline patient characteristics (n=37)

Primary and secondary outcomes (n=37)
Echocardiography results
The echocardiographic variables are reported in Table 3. The mean PASP decreased significantly after TT (56.51±7.34 mmHg vs. 34.16 ±2.81 mmHg, P<0.001) and continued to decrease significantly until discharge (34.16±2.81 mmHg vs. 30.35±3.19 mmHg, P< 0.001). The mean PASP was preserved at the 6-month follow-up visit (28.70±3.04 mmHg), and none of the patients had pulmonary hypertension. The mean TAPSE increased significantly after TT (1.43±0.33 cm vs. 2.07±0.27 cm, P<0.001). The MPI index steadily and significantly improved after TT (0.47±0.08 vs. 0.55± 0.07, P<0.001). The S’ increased significantly after TT (9.6±2.8 cm/sec vs. 15.3±2.6 cm/sec), and the RV/LV diameter steadily and significantly decreased after TT (1.37±0.12 vs. 0.99±0.12, P<0.001).

Echocardiographic outcomes of patients
Treatment complications
No major bleeding events were observed. Three patients had minor bleeding: two patients had epistaxis, and the remaining patient had gingival bleeding. The two episodes of epistaxis were observed 2 days after TT, and the gingival bleeding was observed 3 days after TT. All the bleeding events occurred during heparin infusion, stopped with gentle compression, and did not recur. None of the patients had a stroke or transient ischemic attack during hospitalization. One patient (3.1%) died in the hospital on the 6th day of hospitalization due to a malignant ventricular arrhythmia. That patient had ischemic dilated cardiomyopathy (LV ejection fraction of 20%) and acute on chronic renal failure.
Clinical course
Overall, one patient died in the hospital, and two patients died during follow-up, both with malignancy. Pulmonary hypertension did not develop during follow-up. None of the patients had recurrent deep venous thrombosis, PE, or RV dysfunction during the follow-up period. All patients had a favorable functional class at their follow-up visit. During follow-up after discharge, six of the 34 patients (17.6%) had major bleeding, and two patients (5.68%) had minor bleeding (according to the Thrombolysis in Myocardial Infarction [TIMI] bleeding criteria) due to warfarin.
DISCUSSION
The present pilot study suggests that an extended infusion of low-dose tPA is safe and effective in treating massive PE. TT was associated with a significant early reduction in PASP and improved RV function that were maintained through the 6-month follow-up. Low-dose thrombolysis with extended administration appears to be a promising option in advanced therapy for massive PE and warrants further study in a larger, randomized controlled trial.
Massive PE is a deadly disease with a reported mortality rate of up to 52.4%, which increases to 65% in patients requiring cardiopulmonary resuscitation [3,6]. Although TT can be lifesaving, studies have indicated that only 30% of massive PE patients receive TT [2,3].
Massive PE patients who were elderly or had comorbidities were less likely than others to receive TT, but those who received TT had a lower in-hospital fatality rate irrespective of their age or comorbid conditions [7]. TT-associated complications, especially major bleeding, might be an important factor in this reluctance to treat, and the risk of TT-associated major bleeding does increase with age [8]. Fiumara et al. [9] revealed that major bleeding was more frequent in unstable patients with PE than in stable patients. The most fearful complication of TT is intracerebral hemorrhage. Konstantinides et al. [10] reported that TT was associated with a major bleeding rate of 21.9% in patients with massive PE. Levine [11] reported an 8.4% incidence of major bleeding and a fatal hemorrhage rate of 2.2% in patients receiving TT for PE. The International Cooperative Pulmonary Embolism Registry reported a 3% incidence of intracerebral hemorrhage [3].
Lowering the TT dose might decrease complications. In the MOPETT (Moderate Pulmonary Embolism Treated with Thrombolysis) trial, Sharifi et al. [12] reported that a lower dose of tPA (50 mg) was safe and effective in treating moderate PE without any cases of major bleeding. That study was performed in patients with moderate PE, and TT was administered as a 10 mg tPA bolus followed by a 40 mg infusion over 2 hours. Recently, Ozkan et al. [13] reported that an extended low-dose infusion of tPA (25 mg tPA in 6 hours) was safe and effective in patients with a prosthetic valve thrombosis. Furthermore, that regimen was also safe and effective for pregnant patients with prosthetic valve thrombosis [14]. In their series, no patient who received an extended infusion of low-dose TT had major bleeding. A few case reports in the literature report on the safety and effectiveness of a prolonged infusion of low-dose TT in very elderly patients with massive PE, who have a high bleeding risk and other contraindications to TT [15–18]. No patients in our study had fatal or even major bleeding. Overall, three patients in this study had minimal bleeding 48–72 hours after completing TT and during heparin therapy (likely unrelated to the administration of TT).
TT augments the restoration of lung perfusion, whereas patients treated with heparin have no substantial improvement in pulmonary blood flow [19–23]. The MOPETT trial showed that lower dose tPA (50 mg) decreased PASP more effectively than heparin therapy alone, and that difference remained apparent during long-term follow-up [12]. We found that an extended infusion of an even lower dose (25 mg) of tPA was still effective in both decreasing PASP and restoring RV function. PASP, TAPSE, the RV MPI, and tissue-Doppler–derived tricuspid lateral annulus systolic motion all improved after TT, and those effects were maintained at the 6-month mark. None of the patients developed pulmonary hypertension during follow-up. Furthermore, no recurrent PE occurred in this study population during follow-up.
There were several limitations in our study. Our study is a single-center, nonrandomized, observational study. The absence of a comparison group receiving standard therapy is a major weakness of this observational trial. This study is not a head-to-head comparison between an extended infusion of low-dose tPA and the standard dose regimen for treating massive PE. However, it is a sizable pilot cohort for this specific study population. All patients with massive PE were treated similarly in our hospital. Furthermore, our relatively small sample size might be underpowered to detect relatively infrequent risks.
In conclusion, our pilot study suggests that an extended infusion of low-dose tPA is a safe and effective therapy in patients with massive PE. This protocol was also effective in decreasing PASP and restoring RV function.
Notes
ETHICS STATEMENT
This study was approved by the Institutional Review Board of the University of Health Sciences Ahi Evren Chest Cardiovascular Surgery Education and Research Hospital (No. 2014-02029456), and patients were enrolled after providing informed consent. This study conforms with the principles of the Helsinki declaration and is registered in ClinicalTrials.gov (identifier: NCT02029456).
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: ACA; Data curation: ACA, IG, CYK; Formal analysis: ACA, IG, CYK, SDW; Investigation: ACA, TG, IG, EK, FB, EH; Methodology: ACA; Supervision: ACA; Writing–original draft: ACA, CYK, SDW; Writing–review & editing: all authors. All authors read and approved the final manuscript.
References
Article information Continued
Notes
Capsule Summary
What is already known
Reduced doses of tissue plasminogen activator have shown efficacy for submassive pulmonary embolism but have been associated with side effects such as bleeding.
What is new in the current study
Markedly reduced doses of tissue plasminogen activator may be efficacious for even massive pulmonary embolism without associated bleeding or other side effects.