INTRODUCTION
Death and disability due to out-of-hospital cardiac arrest (OHCA) are a significant public health concern [1,2]. The causes of OHCA can be primarily classified as cardiac and non-cardiac [3]. Many studies have focused on OHCA due to cardiac causes, including ischemic heart disease, because it accounts for a large proportion of cases of OHCA and is the main target of active resuscitation [4,5]. OHCA of cardiac origin is known to share clinical risk factors with coronary heart disease [6,7]. As lipid profile is a significant risk factor for atherosclerotic disease, studies have been conducted to evaluate its association with OHCA [8,9]. Most of these studies have focused on the adverse effects of total cholesterol or low-density lipoprotein (LDL) cholesterol [10-12]. However, only a few studies have demonstrated an association between an unfavorable lipid profile and the development of OHCA [13-15]. Cholesterol is an essential nutrient in the human body that plays a positive role in signal transduction and hormone synthesis [16]. The athero- and cardio-protective effects of high-density lipoprotein (HDL) cholesterol are well known [17]. There is evidence that reduced total cholesterol absorption efficiency is related to all-cause mortality [18]. In addition to the protective effects of high total cholesterol, a study has shown that systemic inflammation and malnutrition associated with lower total cholesterol levels influence mortality [19]. Additionally, several studies have shown that lower cholesterol levels are associated with higher mortality in various diseases and conditions [20-22]. However, few studies have focused on the association between low total cholesterol levels and the occurrence of OHCA; to investigate this, we conducted a case-control study comparing total cholesterol levels between patients who experienced OHCA and a healthy control population. We hypothesized that patients who experienced OHCA would have lower total cholesterol levels than control subjects.
METHODS
Study design and data sources
This case-control study was performed using datasets from the Cardiac Arrest Pursuit Trial with Unique Registration and Epidemiologic Surveillance (CAPTURES) project and the Korea National Health and Nutrition Examination Survey (KNHANES). Cases of OHCA were obtained from the CAPTURES project dataset and controls from the KNHANES dataset. Controls were randomly matched according to age (in 10-year intervals), sex, and county. Matching controls from the same county ensured that the controls were representative of the same source population as the patients. The ratio of controls to patients was 4:1; this ratio was used to increase the statistical power of the study, considering the rare nature of OHCA events [23].
The CAPTURES project database was created from a nationwide prospective multicenter cohort study designed to implement an emergency department (ED)-based OHCA surveillance system in South Korea. It was designed to identify organic problems and risk factors associated with the occurrence of OHCA based on pathophysiology. The CAPTURES project was conducted between February 2014 and January 2015 across 26 EDs. Data for the project were collected from emergency medical service (EMS)-treated patients experiencing OHCA that was suspected to be due to a cardiac etiology by emergency physicians in each ED. The project excluded patients with terminal illnesses, those in hospice care, pregnant patients, those living alone or homeless without a reliable information source, and those with a ŌĆśDo Not ResuscitateŌĆÖ card. Patients who experienced OHCA for whom resuscitation was not attempted in the ED; those transferred between hospitals; and those with a confirmed non-cardiac etiology including trauma, drowning, poisoning, burns, asphyxia, or hanging were also excluded.
The CAPTURES registry includes data on sociodemographic variables, health behaviors, medical history, physical and emotional stress, EMS and ED information presented using the Utstein template, laboratory test results, and cardiac examination results. Emergency physicians at each study site ED collected the information using structured survey papers during a face-to-face interview with patientsŌĆÖ caregivers. Study coordinators at each study site ED collected the results of laboratory tests and cardiac examinations via medical record review. The collected data were inputted and transferred to the central data server at the Korea Disease Control and Prevention Agency (KDCA). The project quality management committee (QMC), which consisted of emergency physicians, cardiologists, and statisticians, reviewed the quality of data via monthly meetings. The QMC trained study coordinators before the project began and guided surveys to ensure that precise information was collected. When the study coordinators were unable to define a coding element, they consulted the emergency physicians in the QMC for clarification.
Community-based controls were selected based on data from the KNHANES collected between 2008 and 2016. The KNHANES is an ongoing national surveillance system based on the National Health Promotion Act that has been conducted annually since 1998 to assess the health and nutritional status of Koreans. This nationally representative cross-sectional survey conducted by the KCDC collects survey sample data from approximately 10,000 individuals each year regarding socioeconomic status, health-related behaviors, quality of life, healthcare utilization, anthropometric measures, biochemical and clinical profiles for non-communicable diseases, and dietary intakes; there are three components to the survey: health interview, health examination, and nutrition survey [24].
Study setting
The Korean EMS is a multi-tier system that offers a basic to intermediate level of life support ambulance services based in fire stations run by the fire department and provided for by the government. Prehospital providers are classified into level 1 and 2 emergency medical technicians (EMTs), comparable to EMT-intermediate and EMT-basic in the United States, respectively. Even if instructed by medical practitioners, EMTs cannot legally perform blood tests in the field, except for blood sugar tests, and point-of-care testing equipment is not available in the Korean EMS. The government designates EDs as levels 1ŌĆō3 depending on the capability and capacity of the facility. In 2014, there were 18 level 1 and 122 level 2 EDs in South Korea; 9 level 1 and 17 level 2 EDs participated in the CAPTURES project. In Korea, blood samples are typically drawn within 5 minutes of arrival at the ED during the early cardiopulmonary resuscitation (CPR) phase [25]. Therefore, several blood test values such as total cholesterol measured in this study were obtained at the hospital stage. Detailed information about the EMS characteristics, OHCA protocols, and ED characteristics has been previously reported [26,27].
Study participants
Cases were defined as adult (age Ōēź18 years) EMS-treated patients who had experienced OHCA with a presumed cardiac etiology and were transported to participating EDs between February 2014 and January 2015. OHCA cases with unknown total cholesterol levels, no information on the presence or absence of dyslipidemia, and those taking lipid-lowering medications were excluded. Controls were enrolled from the KNHANES database. Community controls with unknown total cholesterol levels, individuals who underwent blood sampling without fasting for more than 8 hours, those with no information on the presence or absence of dyslipidemia, and those taking lipid-lowering medications were excluded.
Measurements
The primary outcome was the total cholesterol level (mg/dL). We classified total cholesterol levels into six categories (<148, 148-166.9, 167-189.9, 190-215.9, 216ŌĆō237.9, and Ōēź238 mg/dL) according to the total cholesterol distribution of the KNHANES group (<10th, 10thŌĆō24th, 25thŌĆō49th, 50thŌĆō74th, 75thŌĆō89th, and Ōēź90th percentiles) [28].
The CAPTURES registry contains information on age, sex, county, date of cardiac arrest, initial electrocardiogram results (ventricular fibrillation, pulseless ventricular tachycardia, pulseless electrical activity, or asystole), response time interval, scene time interval, transport time interval, EMS defibrillation attempt, medical history (hypertension, diabetes mellitus, and/or dyslipidemia), and health behaviors including smoking (current smoker, ex-smoker, never-smoker, or unknown), alcohol use (frequent alcohol consumption [more than twice per week], occasional alcohol consumption [once or twice per week], no alcohol consumption, and unknown), number of hours spent sleeping per night (0ŌĆō6 hours, 6ŌĆō8 hours, over 8 hours, and unknown), and body mass index (BMI [kg/m2]; 10.5ŌĆō18.4, 18.5ŌĆō24.9, over 25.0, and unknown) for patients that have experienced OHCA.
When patients who experienced OHCA attended EDs, arterial blood gas analysis and routine laboratory examinations, including total cholesterol measurements, were performed as soon as possible. In addition to total cholesterol, LDL cholesterol, HDL cholesterol, and triglyceride levels were measured if possible. Blood samples were usually collected by nurses at the ED and transported to a central laboratory room where the blood was examined using commercially available laboratory machines. All laboratories involved in this study participate in qualification programs such as the College of American Pathologists survey.
The KNHANES registry contains variables related to participantsŌĆÖ demographics, medical history, health behaviors, and laboratory test components, including total cholesterol, LDL cholesterol, HDL cholesterol, triglyceride level, white blood cell count, hemoglobin level, platelet count, aspartate transaminase level, alanine aminotransferase level, blood urea nitrogen level, and creatinine level. According to standardized protocols, all health examination procedures were performed by trained medical personnel, and all equipment was calibrated periodically. Blood samples were collected from participants aged Ōēź10 years who had fasted for Ōēź8 hours. When LDL cholesterol samples were not obtained using direct assay and total cholesterol, HDL cholesterol, and triglyceride level measurements were obtained, LDL levels were calculated according to the Friedewald equation [29]. When the individualŌĆÖs triglyceride concentration was >400 mg/dL, LDL cholesterol values were treated as missing data because the LDL cholesterol value estimated from the above formula was less accurate. The laboratory data quality control program monitors laboratory performance to ensure that all analytical values meet acceptable standards of precision and accuracy [21]. The lipid panel was categorized and presented based on the KNHANES value. Total cholesterol was categorized according to the 10th, 25th, 50th, 75th, and 90th percentiles, whereas HDL cholesterol, LDL cholesterol, and triglyceride were categorized based on the 25th and 75th percentiles.
Statistical analysis
Demographics of the OHCA patient and community control groups were evaluated. Categorical variables were analyzed using the chi-square test, and continuous variables were analyzed using the t-test when they followed a normal distribution. For missing data on medical history, health behaviors, and laboratory parameters, multiple imputations with multivariable proportional logistic regression models were conducted. In case of HDL cholesterol, LDL cholesterol, and triglyceride levels, multiple imputations were not performed because there were many missing values, and categories were divided according to the distribution of the KNHANES values (the 25th and 75th percentiles). For the matched case-control dataset, multivariable conditional logistic regression analysis was conducted to estimate the effect of the total cholesterol level on the risk of OHCA and to calculate the adjusted odds ratios (AORs) and 95% confidence intervals after controlling for potential confounders identified in directed acyclic graph models. Sensitivity analyses were performed in the cardiac arrest group with a shockable rhythm, the group with a relatively normal pH and potassium levels after cardiac arrest, and the relatively young group without hypertension and diabetes. Statistical significance was defined as a P-value <0.05. All statistical analyses were performed using the SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
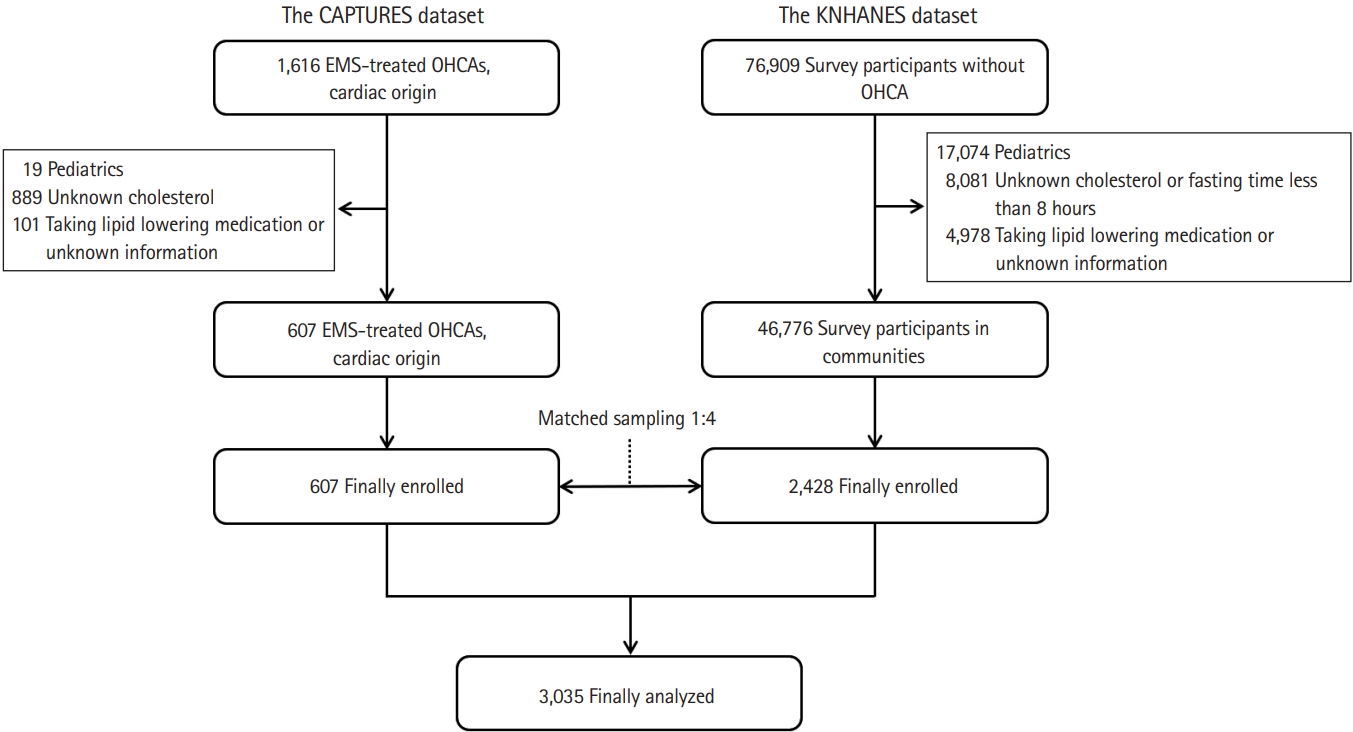
A total of 607 matched case-control pairs were included in our analysis (Fig. 1). Characteristics of the OHCA and community control groups are shown in Table 1. Patients who had experienced OHCA were more likely to have diabetes mellitus and hypertension. The OHCA group had more never-smokers and non-drinkers and had fewer people who rarely exercised, slept less than 8 hours per night, and were obese.
Laboratory findings for patients who experienced OHCA and community controls are shown in Table 2. Patients in the OHCA group were more likely to have lower hemoglobin levels and platelet counts as well as higher white blood cell counts and aspartate transaminase, alanine aminotransferase, blood urea nitrogen, and creatinine levels than the community controls. The OHCA group had lower overall levels of total cholesterol, HDL cholesterol, LDL cholesterol, and triglycerides than the control group. Fig. 2 shows the lipid panel histograms for the OHCA and control groups.
Results of the multivariable conditional logistic regression models, including the AORs (95% confidence intervals), are shown in Table 3. Subjects with a total cholesterol level of 167ŌĆō190 mg/dL (25thŌĆō49th percentile in the KNHANES dataset) were used as the reference group for analysis of the association between total cholesterol levels and each outcome. In both the unadjusted and adjusted models, total cholesterol levels of <148 mg/dL and 148ŌĆō167 mg/dL were significantly associated with the occurrence of OHCA. Potential confounders included BMI, past medical history (diabetes mellitus or hypertension), health behaviors (smoking, alcohol consumption, hours spent sleeping per night, and exercise), and laboratory data (hemoglobin and creatinine levels). BMI, past medical history, health behaviors, and laboratory data used as potential confounders also had significant AOR values (Supplementary Table 1).
Table 4 shows results of the subgroup analysis for patients who experienced OHCA and community controls. We created subgroups for patients with witnessed OHCA and a shockable rhythm, relatively normal values for serum potassium and pH, and those of a relatively young age and no history of diabetes or hypertension. Analysis of the subgroups showed similar results: the lowest total cholesterol group showed a significantly higher AOR.
DISCUSSION
In this case-control study, individuals with low total cholesterol levels were found to have a higher risk of developing OHCA. The results of the analyses indicate that the risk of OHCA increases significantly when the total cholesterol level is less than the national populationŌĆÖs lower 10th percentile.
Recently, several studies on OHCA survivors have reported that the initial serum total cholesterol level is associated with good neurological outcomes [30-32]. One of these studies reported that HDL cholesterol was associated with outcomes following OHCA, whereas LDL cholesterol and triglycerides were not [31]. It has been postulated that cholesterol might influence prognosis following OHCA due to the anti-inflammatory and antioxidant effects of HDL cholesterol [33]. In our study, the lower 25th percentile lipid panel group (HDL cholesterol, LDL cholesterol, and triglyceride level) was associated with a significantly higher risk of OHCA in the multivariable logistic regression analysis (Supplementary Table 2). Therefore, not only low HDL cholesterol but also low LDL cholesterol or triglyceride level may be a risk factor for the development of cardiac arrest [18,19]. Previous studies have reported that low lipoprotein levels are associated with high mortality [34-38]. Our study has shown an association between low cholesterol and an increased occurrence of OHCA, suggesting that low lipid levels may be a risk factor for the development of OHCA.
The calculated total cholesterol cut-off values used in previous studies were 148 mg/dL and 169.5 mg/dL [30,31]. These studies used the Youden index to determine the optimal total cholesterol cut-off value. Our study identified a cut-off value from the distribution of total cholesterol levels across the national population to evaluate the risk of OHCA in the population. The cut-off values calculated in previous studies to determine a good neurological outcome in survivors of OHCA were similar to those obtained in this study when calculating the odds of occurrence of OHCA in the general population. Therefore, total cholesterol may affect the prognosis of OHCA and its occurrence through a similar mechanism.
High cholesterol levels increase the risk of cardiovascular diseases such as atherosclerosis and acute coronary syndrome [39]. Many studies have been conducted based on the hypothesis that unfavorably high cholesterol levels are a risk factor for the development of OHCA, but no clear conclusion has been reached so far [10-15]. Some studies focused on the hypothesis that low cholesterol can cause more cardiac arrests because of the belief that ŌĆśthe lower, the betterŌĆÖ. Our study found that in the general population, those with total cholesterol levels below the lower 10th percentile were at an increased risk of developing OHCA. Consistent results were also obtained when we only analyzed total cholesterol levels in the subgroup analysis. Individuals with low total cholesterol levels may have other chronic diseases or unhealthy conditions that could lead to cardiac arrest, and they may be more likely to develop cardiac arrest for this reason than the total cholesterol level itself. To overcome this bias, we selected a subgroup of patients who experienced OHCA with a relatively ŌĆśsuddenŌĆÖ onset rather than due to slower deterioration associated with a chronic disease.
Hosadurg et al. [8] conducted a case-control study on the effects on sudden cardiac death, with lipid profile as the main variable. They hypothesized that patients with sudden cardiac death would have a less favorable lipid profile than control subjects. However, the OHCA group had more favorable total, LDL, and non-HDL cholesterol levels. This suggested that there is probably no link between traditional lipid cardiovascular risk factors and sudden unexpected death. We believe that these hypotheses and explanations do not clearly distinguish between dyslipidemia and lipid levels. In our study, a relatively higher total cholesterol level was associated with a lower risk of developing OHCA. Patients that experience OHCA do not have a ŌĆśfavorableŌĆÖ lipid profile but are likely to have a dangerously low lipid profile.
In general, LDL cholesterol and triglyceride level are recognized as risk factors for the development of cardio- and cerebrovascular disease. However, the ŌĆślipid paradoxŌĆÖ concept that describes how an individualŌĆÖs prognosis is relatively poor in the presence of a low lipid profile has been proposed in studies of the elderly [40,41] as well as in studies of patients with acute myocardial infarction [42-44], heart failure [45,46], and ischemic stroke [47,48]. In one study, Lopez et al. [49] reported low total cholesterol levels to be associated with a high incidence of atrial fibrillation in the community that they studied. Based on the results of these studies, the total cholesterol level may be related to the development of cardiac arrest.
There are some limitations to this study. First, the possibility of measurement bias should be considered. In the CAPTURES group, the total cholesterol levels were not measured after standardized fasting durations and were measured in different laboratories of each hospital; thus, there is a possibility that they are not uniform and accurate. Total cholesterol levels may have decreased after cardiac arrest. In a canine CPR model, significant changes were noted in total cholesterol values obtained during CPR and at baseline (-16.4┬▒23.6 mg/dL) [37]. In our study, blood was collected immediately after arrival at the ED; thus, the time interval between cardiac arrest and blood sampling was not large. In general, hyperkalemia and metabolic acidosis occur during cardiac arrest [50]. In our studyŌĆÖs sensitivity analysis, the direction of the results did not change even when analyzing the subgroup with relatively normal potassium and pH levels. Unfortunately, the timing of blood collection for the measurement of total cholesterol was not recorded in this study. The CAPTURES project measured the time of serum troponin collection. Serum troponin and total cholesterol were likely collected simultaneously from patients in the OHCA group. The time to collect serum troponin from the estimated time of cardiac arrest was calculated for 482 patients; the average time was 84 minutes, and the median was 57.5 minutes. There was no statistical difference when comparing the distribution of total cholesterol by dividing it into two groups based on a cut-off of 60 minutes (Supplementary Table 3). In addition, there were no clear differences between the total cholesterol distributions of the short prehospital time group (<30 minutes before hospital admission) and the long prehospital time group (Supplementary Table 4). In this study, multiple imputations were applied to the missing values of all variables except the lipid panel. Further analysis was conducted to evaluate the possibility that the estimated missing values had influenced the results. When analyzing the data without imputation, the main results did not change (Supplementary Table 5). The height and weight measurements in the KNHANES registry were performed by nurses belonging to KCDC and underwent quality control. Each hospital conducts height and weight measurements independently in the CAPTURES registry; as this has not been subjected to standard quality control, the accuracy may be relatively low. Second, the possibility of selection bias should be considered. Patients who were not included in the final analysis because of missing cholesterol data were likely to have a different distribution of cholesterol levels. On comparing patients in the OHCA group whose cholesterol levels were measured to those whose cholesterol levels were not measured, no clear differences were noted in any variable (Supplementary Table 6). Third, some diseases that decrease the total cholesterol levels may have acted as confounding variables. Patients who experienced OHCA, were younger than 65 years, and did not have hypertension or diabetes could be assumed to have a relatively good physical functional status; interestingly, the results were the same when a sensitivity analysis was performed in this group. Fourth, data on underlying diseases such as coronary artery disease, which are closely related to OHCA, could not be obtained. If these data were available, these could have been used as a potential confounding variable or as a sensitivity analysis subgroup. Finally, issues related to dyslipidemia should be considered. To control the effects of dyslipidemia treatment, patients taking lipid-lowering medication were excluded from the analysis. Therefore, our study results could not address the risk of OHCA in the population that are treated for dyslipidemia. However, patients with dyslipidemia are likely to have higher total cholesterol levels than the average individual in the general population.
In conclusion, this case-control study demonstrated that having a very-low total cholesterol level was associated with the risk of OHCA. The clinical implication of this study is that low cholesterol levels should be considered important, not only in estimating the prognosis of OHCA survivors but also in predicting the development of OHCA.