INTRODUCTION
Suicide is a global social problem, particularly in Korea. The suicide rate in Korea was 24.6 per 100,000 people in 2019, which is more than double the Organization for Economic Cooperation and Development average suicide rate of 11.0 [1]. Suicide attempts are acts committed with an intent to die that do not cause death but potentially injure the attempter [2]. They are the steps that lead to suicide, and the results range from mild to critical injury, depending on the method and severity of the attempt. In addition to evaluations of the physical injuries, mental health evaluations are required in emergency departments (EDs) whenever patients show an intention toward or evidence of self-injury.
Coronavirus disease 2019 (COVID-19), reported for the first time at the end of 2019, is an infectious disease that has caused a global pandemic, with no effective treatment yet available. A similar global infectious disease before the COVID-19 pandemic was the Spanish flu, which passed through two waves from 1918 to 1920, infecting about a third of the world’s population and killing 50 million people [3,4]. One study reported that fear of infection, isolation, disconnection, and quarantine were associated with increased suicide rates during the Spanish flu outbreak [3].
Before COVID-19, the most recent infectious disease outbreak in Korea was Middle East respiratory syndrome. The first confirmed case was reported in Korea on May 20, 2015, and since then, 186 people were infected, and 38 people died [5]. Of the 1,656 people who were kept in quarantine and received a final negative test, 7.6% complained of anxiety [6]. In a study of those who were infected with Middle East respiratory syndrome and survived, 42.9% had posttraumatic stress disorder, and 27.0% had depressive disorder [7]. Similarly, in a study of 402 survivors of COVID-19 infection, 42% had anxiety, 31% had depression, and 28% had posttraumatic stress disorder [8].
Reports detailing how the COVID-19 pandemic has affected the mental health of the general population are increasing. A study of 1,201 individuals from the general population in China found that 16.5% had moderate depression and 28.8% had moderate to severe anxiety about the COVID-19 pandemic [9]. A larger study of 52,730 people from, China, Hong Kong, Macau, and Taiwan reported a mental distress rate of 35% [10].
In summary, the COVID-19 pandemic is adversely affecting the mental health of the general population, as well as people made vulnerable by preexisting mental illness. Previous studies have dealt with the effects of COVID-19 on mental health, but few have examined suicide attempts associated with the pandemic.
In this study, we investigate the sociodemographic and clinical characteristics of suicide attempters who visited an ED before and during the COVID-19 pandemic.
METHODS
Study design and participants
This study evaluated patients who visited a regional emergency medical center in Gyeonggi Province, Korea. This is a retrospective observational study using the medical records of patients who visited the ED between January 1, 2019 and December 31, 2020. According to the categories of the National Emergency Department Information System, patients that met the criteria for “self-harm/suicide” and were included in our analyses. We excluded patients whose records indicated that they did not attempt suicide and patients from outside the region who were admitted with carbon monoxide poisoning. This retrospective study was exempted from approval by the institutional review board of Myongji Medical Foundation (No. MJH 2021-04-017).
Data
We obtained information about patients’ age, sex, method of suicide attempt, suicide attempt history, presence of mental illness, cause of suicide attempt, occupation, family history, endotracheal intubation, and disposition from the medical records.
Analysis
Counts and percentages were used to present descriptive data. We used chi-squared testing for nominal variables to evaluate differences before and during the COVD-19 pandemic. The odds ratio (OR) values for admission or death were calculated using binominal logistic regression analysis. Data were statistically analyzed using IBM SPSS ver. 27.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at P<0.05.
RESULTS
Participants
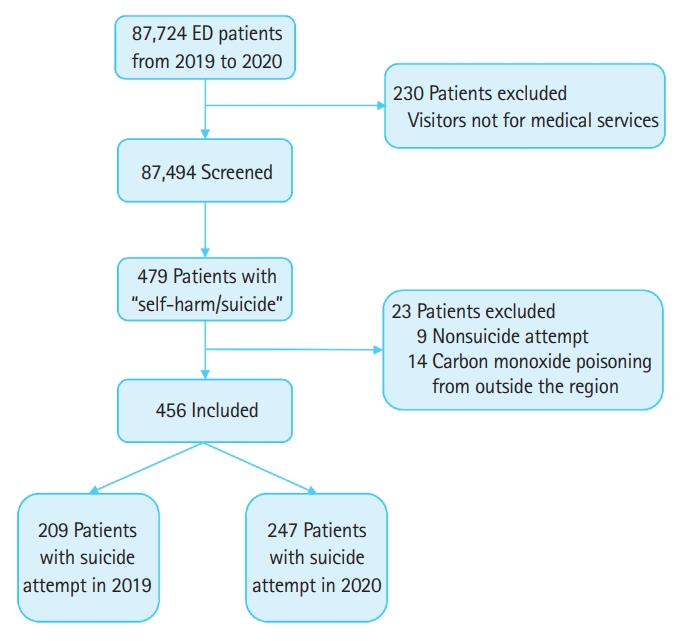
In 2019, 48,915 patients visited the emergency medical center, and that number decreased to 38,809 in 2020. Of the 87,724 patients, 87,494 were screened in this study, excluding 230 who visited for purposes other than medical treatment. Among them, the medical records of 479 patients who met the criteria for “self-harm/suicide” were reviewed. Nine patients whose records indicated that they did not attempt suicide were excluded. Because this emergency medical center started running a hyperbaric oxygen treatment center in July 2020, 14 patients from outside the region who were admitted with carbon monoxide poisoning were excluded. Therefore, 456 patients were included in the analyses (Fig. 1).
Sociodemographic and clinical characteristics
During the COVID-19 pandemic, the total number of patients admitted to the ED decreased by 20.7%. However, the number of patients who visited the ED due to suicide attempts increased from 209 to 247 each year, increasing 18.2% above before-pandemic levels. Additionally, the suicide attempter-to-total ED visit ratio rose from 0.43% to 0.64%, an increase of 48.8% over the before-pandemic levels (P<0.001). Before the COVID-19 pandemic, suicide attempts were most common among people in their 40s and 50s, at 36.8%, whereas during the pandemic, they were most common among those in their 20s and 30s, at 40.1% (Table 1). Among all suicide attempters, 68.2% were in their 20s to 50s. Of the 456 study subjects, 310 (68.0%) were women and 146 (32.0%) were men (Supplementary Table 1). Among women, those in their 20s and 30s accounted for the largest percentage (39.4%), and among men, those in their 40s and 50s accounted for the largest percentage (37.0%).
During the entire period, drug overdose (48.2%) was the most common suicide attempt method, followed by cutting (26.8%), poisoning (including household and industrial materials and pesticides) (9.2%), and gas inhalation (7.2%). There were significant differences in methods of suicide attempt (P=0.001). During the COVID-19 pandemic, drug overdoses increased by 50.0% (from 88 to 132), cutting by 6.8% (from 59 to 63), and gas inhalation by 75% (from 12 to 21). Hanging decreased by 61.5% (from 13 to 5), as did poisoning, 60.0% (from 30 to 12).
Endotracheal intubation was performed in 9.4% of patients, which decreased by 51.7% during the COVID-19 pandemic (P=0.003). As for the disposition of suicide attempters, discharge was the most common at 64.9%, followed by admission to the intensive care unit (21.5%), admission to the general ward (13.2%), and death (0.4%). The number of discharged patients increased by 53.0%, and the number of patients admitted to the intensive care unit decreased by 41.9%, which was strongly correlated with the COVID-19 pandemic (P=0.001).
Of the 456 cases, 173 had insufficient information on sociodemographic characteristics. Of the remaining 283 suicide attempters, 51.6% had a history of suicide attempts, which did not change significantly during the COVID-19 pandemic (Table 2). The number of suicide attempters with a history of mental illness increased by 34.7% during the COVID-19 pandemic (P=0.005). Personal relationships (62.2%) were the most common reasons given for suicide attempts, followed by worsening mental illness (22.3%), economic problems (12.4%), and health problems (3.2%). No significant correlation was observed between any of those reasons and the COVID-19 pandemic. Among the suicide attempters, 52.3% were unemployed, 31.8% were employed, 81.3% lived with their families, and 18.7% lived alone. None of those variables correlated significantly with the COVID-19 pandemic.
Clinical characteristics and their associations with admission or death are shown in in Table 3. Each method showed a significant correlation with admission or death (P<0.001). Hanging (OR, 2.81; 95% confidence interval [CI], 1.05-7.52; P=0.041), taking poison (OR, 3.98; 95% CI, 1.96-8.10; P<0.001), and falling (OR, 3.12; 95% CI, 0.89-11.00; P=0.076) had higher hospitalization rates than the other methods. The hospitalization rate was highest among those in their 60s and 70s (OR, 6.95; 95% CI, 3.07-15.74; P<0.001), and lowest among those younger than 20.
DISCUSSION
Isolation and disconnection are closely related to mental health and are some of the main factors associated with suicide [11]. They include not only the narrow meaning of singleness, divorce, or absence of family or friends but also the broader concepts of loneliness, sense of difference, and lack of social support [12]. During the 2003 severe acute respiratory syndrome epidemic, a study showed that disconnection and isolation were associated with an increase in suicide rates and adverse effects on mental health [13]. The quarantines, social distancing, and lockdowns associated with the COVID-19 pandemic are exacerbating feelings of isolation and disconnection and adversely affecting people’s mental health [14].
Emotional stress is also a significant factor associated with suicidal ideation and suicide. A study of 2,074 students found that depression, anxiety, stress, and despair were important suicide risk factors [15]. A study of 522 teenage patients admitted to an ED in the United Kingdom found that patients reporting recent feelings of anxiety had more than five times the risk of suicide (OR, 5.18) than those who did not [16]. Emotional stress can lead to substance abuse and depression, which can in turn lead individuals to choose suicide as the last way out [17]. The spread of COVID-19 is related to emotional stress [18].
Economic crises and the suicide rate have also been strongly linked. In a case-control study of 538 people in India during an economic crisis, the suicide rate of the unemployed group was six times higher (OR, 6.15) than that of the employed control group [19]. A nationwide study in the United States reported a strong positive correlation between unemployment and suicide rates during the 2007 to 2009 economic crisis [20]. Such positive correlations tend to appear regardless of the income level of a country. The COVID-19 pandemic is associated with an increase in the unemployment rate and economic crises [21].
The COVID-19 pandemic appears to cause isolation, disconnection, anxiety, depression, and stress through the various quarantine policies enforced around the world and economic crises. Those changes were expected to affect the causes of suicide attempts, but we found no statistical correlation between the reported causes and the COVID-19 pandemic in this study. The reasons for this finding are as follows: an individual’s persistent stress leads to psychiatric disorders such as depression, sleep disorders, and adjustment disorders. Subsequently, the psychiatric disorders progress to the stage of suicidal ideation, and exposure to an impulsive situation with a trigger leads to a suicide attempt. In this study, it is unclear whether the cause given for each suicide attempt was a factor causing persistent stress or an impulsive trigger. We thus attribute our finding of no statistical association with the COVID-19 pandemic to the limitation in determining the detailed causes of suicide attempts.
Similar to previous studies in Korea [22], 68.2% of the suicide attempters in this study were young or middle-aged. In this study, the male to female ratio was 1:2.1, with the rate of suicide attempts by women more than twice as high as that by men. The intensive care unit admission rate was higher in those older than 60 years (P=0.001), which was similar to previous studies [23,24]. In addition, the most common causes given for suicide attempts were relationships with others (59.3%) and economic problems (22.1%) in men and relationships with others (63.5%) and uncontrolled psychiatric disease (26.9%) in women. Those results are also similar to those in previous research [25]. In a recent study of 6,816 adolescents who visited the ED due to suicidal ideation or a suicide attempt, female youth and adolescents with no previous psychiatric history were reported to be the most vulnerable group [26]. However, in this study, we find patients with a history of mental illness to be the most vulnerable group. During the COVID-19 pandemic, the number of suicide attempts made by people with a history of mental illness increased by 34.7%, which was statistically significant (P=0.005). We attribute that finding to differences in the representativeness of the sample because the previous study analyzed a large-scale, community-based integrated medical system database, whereas we examined data from a regional emergency medical center with high severity. For example, in the previous study, about 3.2% of all ED patients had attempted suicide, whereas in this study, the rate was only 0.5%.
The changes in the methods of suicide attempts before and during the COVID-19 pandemic are interesting. The lethality of suicide attempts varies with the method used. One study reported that poisoning, hanging, jumping, and gas inhalation had high lethality, whereas drug overdoses and cutting had lower lethality [27]. In another study, the case fatality was 83.4% for hanging, 61.5% for gas inhalation, and 60% for jumping, whereas it was only 2.6% for cutting and 2.2% for a drug overdose [28]. In our study, poisoning, hanging, jumping, and gas inhalation, which are highly lethal methods, decreased by 23.7%, whereas drug overdose, cutting, and suicidal ideation, which are less lethal, increased by 32.7% (P=0.011). The frequency of intensive care treatment and death by suicide decreased by 41.3%, and the rate of intensive care treatment and death by suicide compared with all suicide attempts also decreased by 50.3%, from 30.2% to 15.0%, during the COVID-19 pandemic.
However, we attribute the increased number of suicide attempters and the decreased lethality of their attempts during the COVID-19 pandemic, specifically the increase in drug overdoses, to changes in accessibility and not sincerity. A study of 30 suicide attempters who used gas inhalation reported that their actual suicidal intention was not high even though they chose a method with high lethality [29]. Another study reported no significant correlation between the degree of suicide sincerity and the results of suicide attempts [30]. One study on drug overdose reported that a drug’s toxicity had little effect on drug choice because most suicide attempters had little knowledge about it. The same study reported that committing suicide took less than 30 minutes in more than half of suicide attempters, indicating that the choice is impulsive. Thus, access to drugs and convenience of use greatly influence the drug choices of suicide attempters [31]. The lethality of suicide attempts differs by method, but rather than deliberately choosing a method in consideration of its lethality or prognosis, suicide attempters choose a method impulsively. In other words, accessibility seems to play an important role. In the above-mentioned study on gas inhalation, the suicide attempters reported that accessibility, degree of pain, convenience, and previous media exposure influenced their choice of method [29].
In this study, patients with a psychiatric history tended to attempt suicide with their psychiatric medications (adjusted OR with age and sex, 2.69; 95% CI, 1.61–4.48; P<0.001). This tendency does not reflect low suicidal intention, but easy access to the drugs. For this reason, suicide attempts with low lethality should not be taken lightly.
This study has some limitations. First, as a retrospective study, our information was limited to the medical records. In particular, when the patient was in a coma or their level of consciousness was confused or medically severe, it was difficult to obtain detailed information from them. It is necessary to obtain systematic information about the causes of suicide attempts. Second, if the injury from a suicide attempt was mild, it might be underestimated compared with before the COVID-19 pandemic. During the COVID-19 pandemic, medical resources have been scarce and focused on seriously ill patients [32]. Among those who attempted suicide, those with mild symptoms might have had difficulty accessing medical services. Fear of infection might also have discouraged patients from visiting the ED [33]. A more accurate result could be drawn from a multicenter study that included small and medium-sized emergency medical centers in the region and community mental health care centers. Third, sufficient psychiatric evaluations and interviews were difficult to obtain in the ED because of time and space limitations. In the ED, all patients share an open space with other patients, so in-depth interviews are difficult, and the reliability of interview content is low. In addition, time limitations make psychopathological evaluations difficult, and diagnoses made under the judgment of one psychiatrist can be less accurate than those made by a team. That problem could be overcome by referring patients to a psychiatric outpatient clinic. However, depending on the patient’s will for treatment and the awareness of their family, a referral to an outpatient department might not be followed. Therefore, patients with well-established family support should be told about the importance of careful observation by their family and sufficiently educated about the need for continuing treatment through a psychiatric outpatient clinic. For those without such support, it might be helpful to consider hospitalization.
The COVID-19 pandemic is thought to be having an adverse effect on public mental health, so the demand for mental health care will increase. Because the COVID-19 pandemic is likely to be prolonged, mid- to long-term national and clinical measures are needed. First, it is necessary to develop a simple instrument that can evaluate the sincerity, severity, and recurrence probability of suicide attempts. Such a structured instrument could help to select high-risk patients for referral to tertiary hospitals that can provide emergency psychiatric treatment. It would be particularly useful in small to medium-sized EDs that cannot afford full-time specialists to evaluate suicide attempters. Because time and space are limited in the ED, a self-report method with high compliance and reliability will be useful, so long as no significant difference is found between it and the clinician-reported method [34]. In addition, a previous study reported that postmanagement through a mental health care center after a suicide attempt significantly lowered the suicide rate. Therefore, it is important to refer patients to a community mental health care center after discharge [35]. Suicide attempters should be registered and managed on a follow-up list, and access to a 24-hour suicide crisis telephone counseling service should be provided.
In summary, this study compared the sociodemographic and clinical characteristics of suicide attempters who visited an ED before and during the COVID-19 pandemic. The study showed that during the COVID-19 pandemic, suicide attempts have increased in the ED although the lethality of many attempts is low. These findings suggest that interventions including preventive measures for suicide attempts, screening of high-risk patients, and a postmanagement process for patients with mental health problems are needed.