INTRODUCTION
Low back pain is one of the most common presenting complaints for underlying spinal pathology, and a plain radiograph of the lumbar spine is usually the first diagnostic imaging modality. The “ivory vertebra” sign refers to the radiological appearance of the affected vertebra that looks smooth, white, and ivory-like; however, this is clinically rare. We present a rare case of a female patient who presented to the emergency department with complaints of lower back and was diagnosed with ivory vertebra on plain lumbar spine radiography, leading to further evaluation.
CASE REPORT
A 77-year-old female patient presented to the emergency department with low back pain that had been increasing in intensity over the past 2 weeks. She also complained of occasional lower abdominal pain and feeling bloated. She denied any complaints of fever, weight loss, loss of appetite, or change in bowel habits. She was seen by a general practitioner, who treated her for gastritis with symptomatic medications; however, her symptoms persisted. She had been feeling lethargic over the last 3 days. She had a past medical history of diabetes, hyperlipidemia, ischemic heart disease, hyperthyroidism, and left middle cerebral artery stroke with good functional recovery. She was compliant with her daily medications.
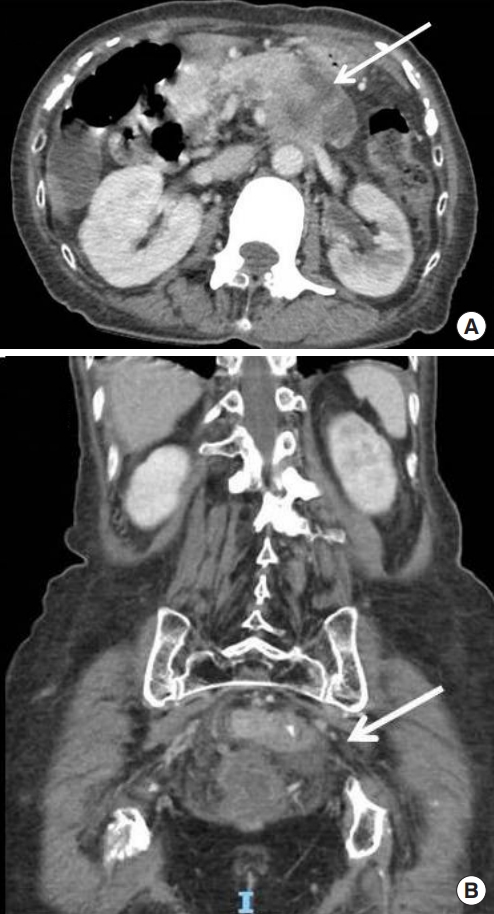
On examination, her vital signs were as follows: heart rate, 117 beats/min; respiratory rate, 17 breaths/min; and blood pressure, 124/82 mmHg. Her abdominal examination was normal. There was no spinal tenderness, and her bedside ultrasound was normal. Blood test results showed a hemoglobin level of 9.4 g/dL and potassium concentration of 3.1 mmol/L. The remaining electrolytes, amylase, and renal panel were normal. Urine examination showed leucocytes. Chest X-ray showed a few nodular densities over the right retrocardiac region and a calcific density over the subcarinal region, representing a calcified lymph node. Anteroposterior (Fig. 1A) and lateral (Fig. 1B) views of the lumbar spinal X-ray showed a diffuse increase in radiodensity and sclerosis of the L2 and L3 vertebral bodies. Computed tomography of the abdomen and pelvis showed short-segment irregular annular mass-like thickening involving the lower sigmoid colon, suspicious for primary colonic malignancy (Fig. 2A), and a heterogeneous mass-like enlargement of the distal pancreatic body with cyst-like hypodensities within, suspicious for either a primary pancreatic malignancy (i.e., adenocarcinoma) with necrotic change or a malignant cystic neoplasm (Fig. 2B). There were associated sclerotic metastases of the L2 and L3 vertebrae. Her CA 19-9 and carcinoembryonic antigen levels were elevated. She was, thus, diagnosed with synchronous pancreatic and rectal malignancy with bony metastases and admitted to the hepatobiliary department for further management. Then, following a discussion of the case at a tumor board meeting, palliative chemotherapy was initiated. The patient, unfortunately, died after 3 months during follow-up. Tha patient’s next of kin provided written informed consent for publication of the research details and clinical images.
DISCUSSION
The vertebral body is normally composed of vascularized trabecular bone, also known as spongy bone. In the ivory vertebra, this trabecular pattern is replaced by homogenous opacification due to the activation of osteoblasts by the underlying disease [1]. This uniform and diffuse sclerosis of the vertebral body gives it a hyperdense appearance. The vertebral body otherwise retains its size and shape, and sclerosis does not involve the adjacent intervertebral discs [2,3]. This increased opacity may either involve a single vertebra or multiple vertebral bodies. In general, a diffuse increase in vertebral bony density is referred to as ivory vertebra, but there are specific imaging characteristics that can point towards an underlying diagnosis. For example, in blastic metastases, the stimulation of osteoblasts leads to irregular replacement of the spinal trabecular bone by amorphous and dense bone masses. The diagnostic characteristics of metastases on imaging are seen as increased vertebral density, multiple spinal level involvement, and blastic lesions in posterior spinal elements.
When radiographs taken to investigate back pain show an ivory vertebra, further evaluation should be performed to look for the underlying causes, the commonest being osteoblastic metastatic carcinoma of the prostate and breast and Hodgkin’s lymphoma [1]. In the elderly, it may also represent metastasis of pancreas and colon cancer, as in our case. It is also seen in Paget’s disease, hemangioma, osteomyelitis, primary osteosarcoma, other skeletal metastasis, sarcoidosis, Pott’s disease, and systemic mastocytosis [4]. It has also been noted in rare diseases like SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome and POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein, skin lesions) syndrome [5,6].
Plain radiographs of the spine and computed tomography scan will show diffuse, homogenous sclerosis of the vertebral body, which looks like ivory, with a variable degree of involvement of the posterior vertebral elements. Magnetic resonance imaging is generally indicated to characterize the details as well as to search for other occult lesions. On magnetic resonance imaging, hypointense, homogenously dark signals of the involved vertebra are seen on both T1- and T2-weighted images, and the intensity is directly proportional to the degree of sclerosis of the vertebral body [2]. Following this, a bone scan can be performed to identify lesions at other sites.
Ivory vertebra is sometimes the initial radiologic manifestation in a variety of infectious, neoplastic, or metabolic diseases. It is, therefore, important for emergency physicians to be aware of this as this will aid in the appropriate evaluation and rapid diagnosis of the underlying disorder.