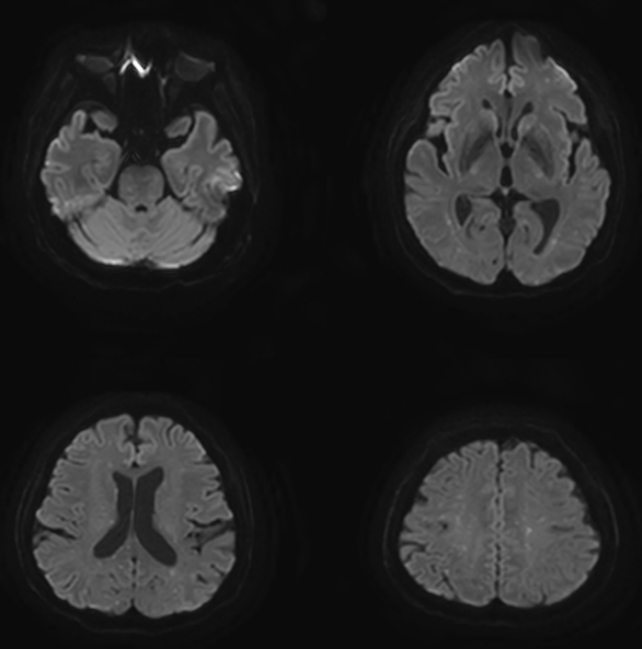
A 69-year-old woman presented to the emergency room with right arm pain after a fall. She was alert and had no other symptoms. She had no relevant medical history. The radiograph showed a right distal radius fracture and fracture of the surgical neck of the humerus (Fig. 1). After 1 hour, she had a sudden change in consciousness, with no response to pain stimulus. Brain computed tomography (CT) was performed immediately but showed no intracranial hemorrhage. Subsequent brain magnetic resonance imaging (MRI) showed multiple embolic infarcts (Fig. 2). In addition, chest CT showed pulmonary thromboembolism (Fig. 3). A second brain MRI performed 2 days after hospitalization showed multiple embolic infarcts with progression (Fig. 4). No evidence of an embolic source was found in the electrocardiogram and echocardiography. The patient remained in a state of stupor mentality throughout the 2-month inpatient treatment. Additionally, the electroencephalogram examination confirmed the presence of epilepsy. After undergoing conservative treatment for 2 months, the patient was transferred to a rehabilitation hospital.
Although histological confirmation was not performed, sudden neurologic deficits, tachypnea, and disseminated intravascular coagulation after long bone fractures strongly suggested fat embolism syndrome (FES), a rare and fatal complication that can occur after a long bone fracture [1–3]. FES usually occurs between 12 and 72 hours postfracture and rarely occurs before 12 hours [2]. This patient developed FES 90 minutes after injury, which is very rare. Neurological symptoms or signs of cerebral FES vary widely, ranging from headache, diffuse encephalopathy, aphasia, and seizures [4,5]. FES should be considered in the differential diagnosis of patients with sudden changes in mental status immediately after a long bone fracture.