INTRODUCTION
Epinephrine, a sympathomimetic agonist acting on α and β adrenergic receptors, exerts direct effects on various target organs. Among the multiple actions of epinephrine, its effects on α1 adrenergic receptors, including vasoconstriction, increasing peripheral vascular resistance, and decreasing mucosal edema, as well as its effects on β2 adrenergic receptors, including increasing bronchodilation and decreasing mediator release by mast cells and basophils, are crucial in anaphylaxis treatment [1]. Epinephrine has been widely used as a first-line drug for anaphylaxis, and its dosage and administration have been documented in several studies [1–3]. If appropriate treatment is not promptly administered, anaphylaxis can progress to a fatal condition; therefore, it is necessary to administer epinephrine before arriving at the hospital, as soon as possible [4].
However, administration of drug concentrations above the therapeutic range can result in pharmacological side effects, such as anxiety, fear, and headache; moreover, rare occurrences of ventricular arrhythmias, myocardial infarction, pulmonary edema, and cerebral hemorrhage have been reported [5].
In this case report, we present a case where inappropriate intravenous epinephrine administration led to atrial fibrillation in prehospital anaphylaxis patient treatment.
CASE REPORT
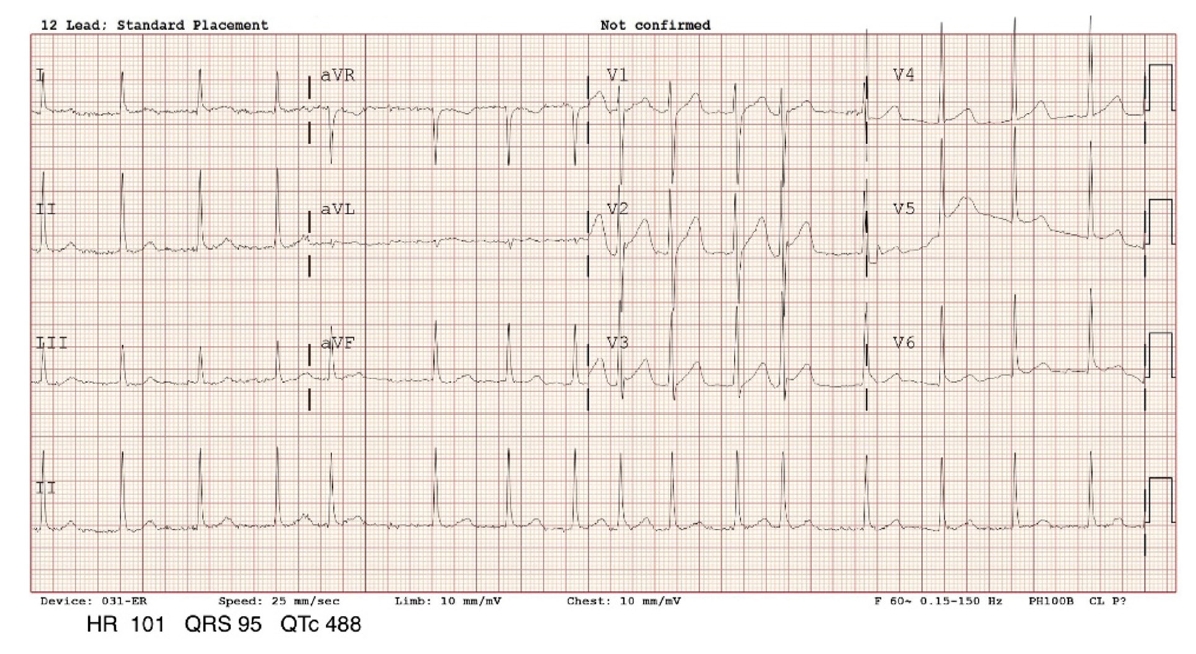
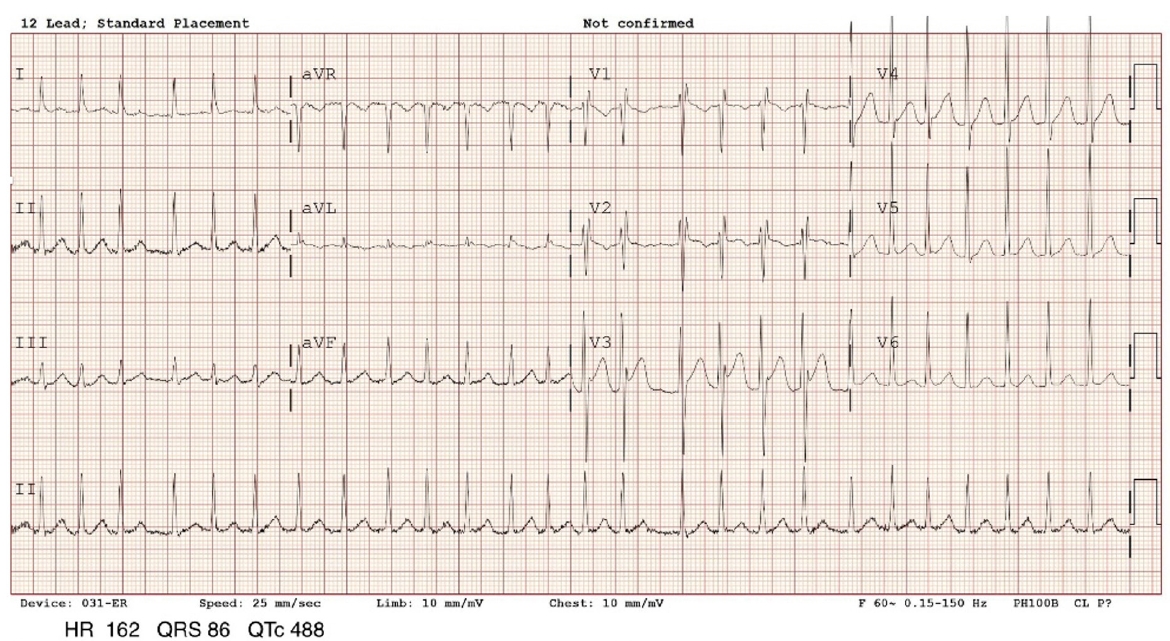
A 46-year-old man presented with respiratory distress, which prompted a call to the public emergency medical services (EMS). The caregiver of the patient reported that he had no significant past medical history or known allergies. On the day of the incident, the patient had visited a primary care facility for sore throat and was prescribed amoxicillin, acetaminophen, pseudoephedrine, ambroxol, and levocetirizine, which were taken at home. Subsequently, dyspnea developed. The patient was found lying on the living room floor by EMS in a drowsy mental state. Vital signs were as follows: blood pressure, 70/40 mmHg; pulse rate, 91 beats/min (bpm); respiratory rate, 14 breaths/min; body temperature, 36 °C; and oxygen saturation (room air), 96%. Emergency medical technicians (EMTs) diagnosed anaphylaxis based on physical examination and assessment results. Under the EMS medical director’s oversight, the EMTs administered 0.5 mg of intramuscular epinephrine (1:1,000) without using an autoinjector and provided 1 L of normal saline, 12 minutes after initial patient contact. Ten minutes following intramuscular epinephrine administration, symptoms had not improved. The vital signs were as follows: blood pressure, 63/27 mmHg, indicating persistent hypotension; pulse rate, 74 bpm; respiratory rate, 18 breaths/min; and oxygen saturation, 99%. Direct medical oversight was requested again, and the EMS medical director instructed a bolus injection of 0.5 mg intravenous epinephrine (1:1,000). One minute following bolus intravenous epinephrine administration, the patient complained of chest pain and palpitations, with the following vital signs: blood pressure, 189/84 mmHg and pulse rate, 179 bpm. After 5 minutes, the patient was transported to the emergency department of a nearby tertiary hospital and immediately moved to the resuscitation room. Upon hospital admission, the patient reported chest discomfort but no other symptoms. His vital signs were as follows: blood pressure, 132/98 mmHg; heart rate, 108 bpm; respiratory rate, 22 breaths/min; temperature, 36.2 °C; and oxygen saturation (room air), 97%. Electrocardiogram (ECG) revealed atrial fibrillation with a heart rate of 101 bpm (Fig. 1). Initial laboratory data showed normal complete blood count, elevated lactic acid level (1.9 mmol/L), and normal high-sensitive cardiac troponin I (hs-cTnI) level (<2.5 pg/mL). Three hours following admission, the hs-cTnI level increased to 141 pg/mL. The patient continued to complain of chest discomfort, and a follow-up ECG confirmed atrial fibrillation with a rapid ventricular rate (Fig. 2). Consequently, amiodorone was administered, which resulted in conversion to a sinus rhythm (Fig. 3). Afterward, the patient did not report any specific discomfort and remained hemodynamically stable with normal blood pressure and without refractory hypotension. The patient was discharged after one day of observation in the hospital, during which he complained of no specific discomfort and his vital signs remained stable. Follow-up ECG revealed a normal sinus rhythm, and the hs-cTnI level decreased to 61.01 pg/mL. Transthoracic echocardiography was performed, which showed no significant cardiac structure abnormalities. One week following discharge, a drug hypersensitivity test performed in the outpatient department showed a positive result for penicillin allergy, confirming that the anaphylaxis episode was triggered by the amoxicillin administration.
DISCUSSION
In anaphylaxis management, epinephrine is recommended as the promptly administered first-line drug. For teenagers and adults, intramuscular administration of a dose of 0.01 to 0.5 mg/kg of body weight (1:1,000) of epinephrine is recommended [2,3]. If symptoms are refractory, repeat doses can be administered at 5- to 15-minute intervals. Most patients respond to one or two doses [2,3]. Intravenous epinephrine bolus administration is not routinely recommended as it can induce fatal arrhythmias [2,3,6–8]. A case of cardiac arrest occurred following intravenous administration of 0.3 mg epinephrine (1:1,000) in a patient with computed tomography contrast-induced anaphylaxis [9]. In a study comparing routes of epinephrine administration in anaphylaxis, intravenous bolus epinephrine had significantly higher risk of overdose and adverse cardiovascular events compared to intramuscular epinephrine administration [6]. However, if used, intravenous epinephrine should be administered by healthcare professionals with experience in diluting and administering correct doses using an infusion pump for monitored patients [3].
Anaphylaxis caused by allergic reactions requires immediate intervention to prevent progression to a fatal condition. Patients with a known history of allergies may have access to an epinephrine autoinjector. However, in cases of initial allergic reactions or reactions triggered by environmental factors, immediate treatment of symptoms may not be possible and initial management may be performed by EMS [10]. In situations where the transportation time to the hospital is short, one or two doses of medication may be sufficient, reducing the need for additional interventions. However, it is essential to be prepared in cases where the transportation time exceeds the timeframe of one or two intramuscular epinephrine doses, and knowledge on the management of anaphylaxis unresponsive to epinephrine administration may be necessary. EMTs play multiple roles from assessing the patient to providing initial treatment and facilitating transport [11]. A previous meta-analysis [12] showed a low rate of epinephrine use in the prehospital setting owing to the fear of potential adverse effects associated with epinephrine injection.
In Korea, the use of epinephrine by EMTs in the prehospital phase for patients with anaphylaxis was legally prohibited. However, due to the necessity of prehospital epinephrine administration in patients with anaphylaxis, a pilot program was initiated in 2019. This project, organized by the Ministry of Health and Welfare and the National Fire Agency, aimed to evaluate the safety of patients following an expansion of EMTs’ scope of practice. Under the EMS medical directors’ oversight through video medical guidance, EMTs who completed education in advanced cardiovascular life support involving epinephrine use in anaphylaxis were permitted to administer epinephrine via an autoinjector to patients with anaphylaxis when deemed necessary. The implementation of this program sought to ensure patient safety while expanding the responsibilities of EMTs [13].
Additional interventions by the EMS medical director would be needed in cases of anaphylaxis, wherein some patients are unresponsive to the initial treatment. A case was reported in Australia [14] wherein an error following intramuscular epinephrine administration by EMTs led to inadvertent administration of 5 mg intravenous epinephrine, which resulted in ventricular tachycardia. In our case, under the medical director’s oversight, EMTs administered not only 0.5 mg of epinephrine intramuscularly without using an autoinjector, but also an intravenous epinephrine bolus. There were discrepancies with the established guidelines for prehospital anaphylaxis treatment. Administering an intravenous epinephrine bolus, even without mentioning deviation from the guideline, was also incorrect. The correct approach involves administering a diluted dose slowly over 5 to 10 minutes in a closely monitored hospital setting [8]. In the prehospital phase, there are limitations in terms of personnel and confined spaces where medical interventions must be performed, which may hinder real-time feedback and communications. To address this, training on the optimal anaphylaxis treatments for EMTs and EMS medical director's sufficient knowledge and careful instruction regarding epinephrine use are necessary. Additionally, adherence to guidelines is crucial.